CREDIT: THEO WARGO/GETTY; NED DISHMAN/NBAE VIA GETTY
Rapinoe said that efforts in Mississippi to enact a highly-restrictive abortion ban were “infuriating and un-American”
More than 500 athletes, including soccer and basketball stars Megan Rapinoe, Diana Taurasi and Sue Bird, filed a lengthy and persuasive brief to the Supreme Court urging them to protect abortion rights as they prepare to hear a case that could overturn Roe v. Wade.
This December, the Supreme Court is scheduled to hear oral arguments on an appeal of a lower court’s decision to block Mississippi’s law banning abortion after 15 weeks of pregnancy. With the conservative-leaning court, the justices could decide in favor of Mississippi, upending the protections of Roe v. Wade, which in 1973 established the right to abortion through 25 weeks of pregnancy.
The brief, which was signed by athletes and sports groups and included 26 Olympians and 73 active professional athletes, argues that access to abortions has helped women’s sports succeed.
Without access to abortions, they wrote, “women’s participation in athletics would suffer, including because some women athletes would not be able to compete at the same level—or at all — without access to abortion care and without the knowledge that the decision whether to continue or end a pregnancy remains theirs.”
“As women athletes and people in sports, we must have the power to make important decisions about our own bodies and exert control over our reproductive lives,” the Olympic gold medalist and two-time World Cup champion said.
Another signatory, Crissy Perham, a three-time Olympic medalist in swimming, shared with The New York Timesthat she had an abortion as a college sophomore, and said that her career would not have been what it was without terminating her pregnancy.
“Ending my pregnancy, I made a decision about which direction to take my life in,” Perham said. “Someone else might decide to go in another direction, and that’s fine. But this was the best decision for me.”
Perham, who won back-to-back-to-back NCAA titles after her abortion and made the 1992 Olympic team, where she won two gold medals in relay races and a silver in the 100-meter butterfly, said that her story is “not uncommon” among athletes.
Along with Rapinoe, Taurasi, Bird and Perham, Ashleigh Johnson, the first Black woman on the U.S. Olympic water polo team and a Tokyo Olympian, signed the brief, as did the player’s unions of the WNBA and the National Women’s Soccer League.
The signers “believe that, like themselves, the next generation of women athletes must be guaranteed bodily integrity and decisional autonomy in order to fully and equally participate in sports.”
Volunteer clinic escorts at EMW Women’s Surgical Center, Kentucky’s only independent abortion clinic, are regularly subject to harassment. Jon Cherry/Getty Images
The Supreme Court will weigh in on a relatively wonky issue, but abortion advocates say the stakes are still incredibly high for the people in Kentucky.
You may know Daniel Cameron as the man who declined to recommend homicide charges for the police officers who killed Breonna Taylor. But Kentucky’s Republican attorney general is also the reason why the Supreme Court will hear an abortion-related case this month, the first abortion-related case in this new term under its 6-3 conservative supermajority. That’s right, the high court has two abortion cases on its docket so far, not just the high-profile Mississippi one in which the state flat-out asked the Court to overturn Roe v. Wade.
The Kentucky case, Cameron v. EMW Women’s Surgical Center, has gotten less attention because the stakes in the Mississippi case are so high and because of the legal chaos in Texas. Moreover, the Court is weighing in on a relatively wonky issue here: whether Cameron can intervene to defend a law after both a district court and an appeals court found it unconstitutional, and after the state’s Democratic administration declined to appeal that decision. The justices are not considering the merits of the anti-abortion law itself.
But don’t let anyone tell you this case is unimportant procedural stuff.
“Even though the legal question doesn’t have to do with abortion, the stakes here are still incredibly high, especially for people in Kentucky,” said Alexa Kolbi-Molinas, senior staff attorney with the American Civil Liberties Union’s Reproductive Freedom Project, who will argue the case on October 12.
The law Cameron wants to defend is a ban on the most common abortion procedure used after 15 weeks of pregnancy, known as dilation and evacuation (D&E). “If the Supreme Court sides with Attorney General Cameron, then he will get to pursue his goal, which is to overturn the underlying decision striking down the abortion ban,” Kolbi-Molinas told Rewire News Group.
If Cameron is able to intervene and the law gets upheld, it could effectively ban abortion after 15 weeks in a state that has just two clinics and multiple restrictions, including a 24-hour waiting period and bans on insurance coverage of the procedure. Both clinics are in downtown Louisville, which means access is limited for people in other areas of the state.
The plaintiff in the case is EMW Women’s Surgical Center, the state’s only independent abortion clinic and the only one that provides care after 14 weeks of pregnancy. Kentucky’s other clinic, a Planned Parenthood health center, was granted a license in January 2020 and offers care through 13 weeks and 6 days, so the D&E ban would not affect it. The Ohio Policy Evaluation Network (OPEN) estimated that EMW provided nearly 90 percent of abortions in the state between March and December 2020, since the clinic provides care more days per week and later in pregnancy.
EMW has been the state’s only clinic for long stretches of time, and it gets targeted by protesters both for that reason and because of its setup, said Meg Sasse Stern, who has been a volunteer clinic escort for more than 20 years. EMW is on a main thoroughfare with no on-site parking for patients, so they have to park elsewhere and walk through the front door, often through a gauntlet of protesters who may try to block their path, grab them, or hand them anti-abortion pamphlets or baby booties, Stern said. An anti-abortion “crisis pregnancy center” right next door offers free parking to EMW patients in an effort to get them inside. In 2017, EMW was the site of the first clinic blockade in almost 15 years, orchestrated by the extremist anti-abortion group Operation Save America. Staff are routinely harassed with threats of harm and hate mail, and, in April 2020, a bomb threat, according to OPEN.“I cannot ignore the vast difference in treatment received by these anti-abortion protesters and the way that our police department treats protesters that are demanding police stop killing Black and brown people.” -Meg Sasse Stern, volunteer clinic escort
By contrast, Planned Parenthood’s health center has a parking lot and a privacy fence around the property, Stern said. “The protesters do not have the same kind of access to the patients [at Planned Parenthood],” said Stern, who is also the support fund director for Kentucky Health Justice Network, a reproductive justice nonprofit that pairs abortion patients with a case manager and helps them pay for their procedure, transportation, lodging, childcare, and other expenses. “They see EMW as low-hanging fruit.”
Ona Marshall, who co-owns EMW with her husband Dr. Ernest Marshall, said protesters and state lawmakers are always targeting their clinic, but “I think in general, they just want to abolish abortion and access to abortion, so they go through the series of laws to see what they’ll be able to do.”
In May, the Louisville Metro Council voted to create a safety zone around the clinic entrance, and the 10-foot buffer zone was implemented in mid-September. Marshall said advocates pushed for the safety zone because of the lack of enforcement of various city ordinances regulating things like harassment, noise, and sidewalk access. She also noted that these same ordinances were enforced against social justice protests after Breonna Taylor’s death, and the Louisville Metro Police Department is now under a pattern and practice investigation by the U.S. Department of Justice. LMPD arrested the state’s only Black woman lawmaker, state Rep. Attica Scott, during a September 2020 protest.
“Anti-abortion protesters are ignored and just treated differently than other protesters,” Marshall said. Stern agreed that the difference is obvious: “I cannot ignore the vast difference in treatment received by these anti-abortion protesters and the way that our police department treats protesters that are demanding police stop killing Black and brown people.”
Both Marshall and Stern are skeptical that the safety zone around EMW will be enforced due to anti-abortion sentiments in the police department. During an August 2020 Metro Council meeting about the proposed safety zone, former council member David Yates, now a Democratic state senator, said he received text messages from police officers asking, “who’s going to enforce this – lol.”
In February, an off-duty officer parked his LMPD cruiser in front of the clinic and protested for about two hours with a “pray to end abortion” sandwich-board sign over his uniform and his gun visible, Stern said. The department placed the officer on administrative leave while investigating the incident, but he was ultimately not disciplined because LMPD hadn’t been consistently enforcing its protesting policies. LMPD said it would require strict compliance going forward.
Stern said the behavior that LMPD tolerates outside the clinic is a public safety risk. “The environment that exists down there just welcomes this kind of extreme behavior where we get these national extremists,” she said, adding that John Brockhoeft, a convicted clinic arsonist who attended the January 6 insurrection, is a regular at EMW.
Like Stern, Marshall is worried that violent protesters feel empowered. “During the last five years, we have experienced a significant and sustained increase in the types of anti-abortion harassment, and those are the types of harassment that have led to tragic outcomes in other cities, so it is something to really pay attention to,” she said.
But not a lot of people are paying attention to either the protesters or the Supreme Court case. “In general in Kentucky, and probably in other states, I don’t think there’s a high level of knowledge about this case,” Marshall said.
And with many people checked out, Cameron is pursuing this piece of his “concerted strategy” to push abortion access entirely out of reach without much fanfare, Kolbi-Molinas of the ACLU said. When the Supreme Court announced it would take Dobbs v. Jackson Women’s Health Organization, Mississippi’s direct challenge to Roe, this Kentucky case got somewhat overshadowed.
“Not wrongfully, not malice or anything like that—but the legal question isn’t about abortion,” Kolbi-Molinas said. But remember: “There is more than one case on the Supreme Court’s docket this term that implicates abortion access.”
A security guard outside the Whole Woman’s Health Clinic in Fort Worth, Texas, on Sept. 1. (LM Otero / Associated Press)
It’s been nearly a month since our country’s cruelest abortion ban went into effect. As of midnight Sept. 1, most Texans seeking abortion care have been left powerless and afraid. Providing abortion care in Texas was difficult before, but now we are living in a dystopian nightmare. Let me share what it was like on the night of Aug. 31 at Whole Woman’s Health of Fort Worth.
In the hours leading up to midnight, the waiting room was filled with patients hoping to get an abortion before Senate Bill 8 went into effect. Staffers and doctors had been working since 7:30 a.m., and they were still there providing abortions until 11:56 p.m. Outside, the antiabortion protesters kept us under tight surveillance all day long. Come nightfall, they shined flashlights into patients’ cars, the clinic and the parking lot. Inside the clinic, there was love, support, bravery, integrity and deep commitment to human rights. We held out hope that the Supreme Court would bar the law from going into effect. But that justice never came.
Today, it is illegal to provide abortions after about six weeks in Texas. Whole Woman’s Health and Whole Woman’s Health Alliance clinics are still open and providing abortions, but every day we turn away most people who need abortion care. We provide abortions for the few we can help — those who are lucky enough to make it in under the narrow limit. Six weeks pregnant means just two weeks past your missed period. As for those who are denied care? They are stunned, numb, frozen.
This law goes against everything we believe in. It prevents doctors from treating patients and turns Texans’ care over to self-appointed vigilantes who are encouraged by a bounty reward system. We’d prefer to defy this unjust ban, but SB 8 is far too terrifying. Our staffers are being surveilled constantly — from the protesters on our sidewalks to the threatening phone calls we get every day. People who are eager to sue us send fake patients into our clinics to see if we will break the law. Our nurses, medical assistants, and counselors are alert, afraid, anxious, worried, and in fear. Many of our physicians have opted out of providing care while SB 8 is in effect. It is just too risky for them. It is a horror tale.
SB 8 puts incredible power into the hands of people who have terrorized us and our patients for decades. And lawmakers in other states are already following in Texas’ footsteps. The Florida Legislature recently introduced a copycat bill, hoping to severely limit abortion access the same way as Texas. There is no saying where this will stop.
SB 8 comes on top of layers of restrictions on people’s access to abortion in Texas. For the last two decades, Texas politicians have imposed forced ultrasounds, a ban on using Medicaid or insurance, two-visit requirements, a mandated 24-hour waiting period, operational regulatory schemes, a ban on a standard abortion method, gestational limits, ambulatory surgical centers facility standards, etc. As if this wasn’t enough, just over a week ago a ban on medication abortion after 49 days was signed into law, and it’s set to go into effect Dec. 2.
I founded Whole Woman’s Health in 2003 in Texas because I believe all people — no matter where they live — deserve access to quality abortion care that is delivered with respect and dignity. We take on the shame and stigma that has been created by those who oppose abortion and defend this constitutionally protected right against political interference and intimidation. I now operate four clinics in Texas and five more across the South and the Midwest — where compassionate care is needed most.
Over the last 18 years, the hurdles to operate abortion clinics in Texas have become mountains. We fought against insidious attacks like SB 8 before. In fact, we won our 2016 case, Whole Woman’s Health vs. Hellerstedt, at the Supreme Court. But clinics can’t fix all these problems alone. If clinics close because SB 8 is enforced long enough to drain all our resources, the damage will be done even if it is eventually struck down.
So, why should all Americans care? Because what happens in Texas rarely stays in Texas. Texas is a barometer for abortion care in this country — Roe vs. Wade was also a Texas case. The truth about Texas? SB 8 does not reflect Texas values or the feelings and beliefs of most Texans. Yet the powerful few have weaponized abortion stigma into laws like SB 8.
And let’s be clear — there are no “safe haven” states for people who need abortions, only states with fewer barriers. Even in states such as California or New York, with state law protections for abortion, many who need care can’t travel the distance to the nearest clinic, or can’t afford the cost of their care, or can’t take time from work or find child care for their kids.
Millions of people — men and women — have benefited from access to abortion in this country. Abortion bans like SB 8 rob us of our ability to make decisions about our lives and futures, to support our families, to pursue our dreams, to remain safe and whole, to be healthy. The people of Texas are suffering every day this law stays in effect.
The man who masterminded the Texas SB 8 strategy for undermining Roe v. Wade listed Alliance Defending Freedom on his disclosure of former income sources. Jordan Vonderhaar/Getty Images
Alliance Defending Freedom is the incubation center for this type of legal approach to dismantling protections around LGBTQ and reproductive rights.
The far right has long played a game of bureaucratic whack-a-mole as part of its efforts to roll back civil rights gains. This includes flooding legislative offices with calls from constituents on mailing lists, flooding the lower courts with experimental lawsuits filed by former Blackstone fellows, and refusing to give up when laws are repealed as unconstitutional. Their determination to weasel through loopholes resembles the pedantic genius of a 7-year-old who doesn’t want to go to bed yet—what if I play the rules this way? How about that way? The endurance is formidable.
Alliance Defending Freedom is the incubation center for this type of legal approach to dismantling protections around LGBTQ and reproductive rights. Founded in 1994, ADF funnels young Christian law students through their Blackstone Legal Fellowship and teaches its particular strategy for dismantling LGBTQ protections and pro-choice laws, a strategy that’s been used to great success in cases like Masterpiece Cakeshop v. Colorado. ADF connections show up in every branch of the federal government, thanks to years of slow work to gain footholds over the last 30 years. Supreme Court Justice Amy Coney Barrett and Sen. Josh Hawley of Missouri both have close ties to ADF through Blackstone.
Because ADF affiliates show up in nearly every big case like this, when the Texas near-total abortion ban passed into law I immediately went to look up the man who masterminded its particularly appalling strategy for undermining Roe v. Wade, and sure enough—there was ADF on his list of former income sources, revealed in the financial disclosures he had to submit when he was nominated for a position in the Trump administration.
Now, this tells us nothing about where the idea for SB 8 came from in particular, though we learned a bit more about that in the last few weeks. But it does tell us who exactly is supporting the people creating these novel legal approaches.
Texas SB 8 is set up to evade the privacy protections that Roe v. Wade is based upon in part by deputizing citizens to enforce its prohibition on abortion once cardiac activitity is detected. The law employs gossip and experiential observation to allow a civil suit to be levied against anyone who is known to have performed or aided an abortion in violation of SB 8.
The fun part about this bill is that the government doesn’t have to pay for these lawsuits—the minimum $10,000 bounty and associated court fees have to be paid by the defendant if they lose the suit. SB 8 sets up scenarios where similar cases could be filed in every county in Texas against a single abortion provider, by multiple plaintiffs, and the provider would have to pay to defend themself in all those cases.
This is interesting, because it appears to be an attempt to avoid situations like the North Carolina “bathroom” law from a few years back, which posed the problem of: If lawmakers are making it illegal for trans people to use the bathroom consistent with their gender, how the hell will they enforce it? With cops performing genitalia checks at restroom doors to ensure that everyone is using the room with stalls that matches their assigned sex?
Tennessee lawmakers are facing a similar logistical nightmare with their new bathroom laws targeting trans access to facilities. The use of surveillance and the invasion of medical privacy to criminalize medical autonomy around gender and reproduction is so contrary to basic American values that it’s difficult to imagine these attempts working long-term. It’s a running issue of enforcement logistics when any of the trans-kids-in-sports bills get brought to a state house floor. How can you enforce such a requirement without essentially groping children on the soccer field? What is necessary to prove that someone meets such a regulation, and how will it be enforced? Who will be checking up on it and making sure that the law is followed? Such questions ended up getting the North Carolina bathroom bill defanged, and eventually aged out of effect.
The reality is, though, that this new Texas law—despite attempts to use civil court proceedings to sidestep logistical challenges around enforcement—is still quite vulnerable to these same lines of challenge. What’s to prevent every abortion rights supporter with means from filing a lawsuit in every county in Texas against, say, the attorney general of Texas, accusing him of aiding and abbeting an abortion? A lawsuit might prove those allegations to be false and the attorney filing the lawsuit might find themselves subject to financial sanction, but the resulting flooding of an already oversaturated legal system that’s fallen even further behind thanks to COVID-19 would be a nightmare of bureaucratic logistics.
These cases would almost certainly be thrown out as a waste of the court’s time—but what if not all of them were? What if the volume was so overwhelming that the legislature would have to step in and amend the law, defanging its ridiculous scope? The fact that such a strategy might actually work is testament to the failure of the pro-abortion left to strategize on the same level as the right by trying everything that might stick. The pragmatism of blunt strategic force seems to be working.
Ultimately, ADF and similar right-wing groups are succeeding with their strategy of overwhelming our civil systems as a substitute for having the will of the people on their side.
Their strategy—swamping state legislatures with increasingly draconian copycat legislation, and flooding federal courts with bogus “religious liberties” cases attacking civil rights gains—is rapidly rewriting civil rights law and undoing decades of progressive progress. Similar bills will be brought to the floor in other states next year, for certain. But the thing is: When pedantry is the game, both sides can play.
The recent Texas law is part of an onslaught years in the making—yet few heeded the warning.
In Sept. 1, Senate Bill 8 went into effect, banning abortions in the state of Texas after about six weeks of pregnancy with nearly no exceptions, becoming the most restrictive abortion law in the nation. The Supreme Court, with its conservative majority, failed to block the law, so even with a Democrat in the White House and a Democrat-led Congress, millions of women and transgender and non-binary people had their rights stripped away from them like a thief in the night. But for those who have been paying attention to the changing Court and as state-level lawmakers have consistently worked to restrict abortion access, especially over this past year, the news from Texas comes as little surprise. It was an onslaught years in the making, yet few heeded the warning.
Reproductive justice leaders on the front lines have long been sounding the alarm about conservatives consolidating power at the state level, leading to this year’s widespread attacks on abortion access and voting rights. Now, with the midterms fast approaching, we can’t afford to lose voters to burnout and disillusionment. Instead, we have to listen to the leaders who’ve been working around the clock to ensure people have safe and destigmatized access to healthcare. We have to have a new, robust, mainstream conversation about reproductive justice—about where we are failing and where we can still succeed. We have to ground people in the true stakes of this fight and make clear who will be most affected by these restrictive policies. Regardless of the outcome of any one election, we must always be out in the streets, participating in and advocating for the future we want.
To do so, ELLE.com brought together four Black and Latinx women who’ve all had a front row seat to the national struggle for abortion care—and have been directly impacted themselves. Below, these healthcare consultants, advocates, and practitioners discuss the devastating effects of this Texas law and what we can do now to change course.
What was your initial response when the Supreme Court failed to stop this Texas law?
COURTESY
Angela Doyinsola Aina, MPH, co-founder and executive director of the Black Mamas Matter Alliance: At the root of this racist, heteropatriarchal law is white supremacy. SB 8 not only prohibits most abortions after six weeks of pregnancy but also empowers individuals to sue anyone who aids or abets a person accessing an abortion, including doctors, staff, drivers, and other community members. We know that Black mamas, their families, and communities will face the most dire consequences as a result of these types of laws that restrict their fundamental rights to comprehensive reproductive and maternal healthcare.
All of a sudden, your friends and family are debating the morality of abortion on your timeline or in your group chats, sometimes not knowing they too know someone who has had an abortion.
COURTESY
Ana Lucia Carmelo, MPH, healthcare consultant, public health advocate, and proud Peruvian immigrant: We know that abortions continue to happen even when they are not legal, and these type of bans disproportionately impact the underserved. It can be easy to feel hopeless, and events like this are especially triggering for people who have had abortions. All of a sudden, your friends and family are debating the morality of abortion on your timeline or in your group chats, sometimes not knowing they too know someone who has had an abortion. That being said, I always think about the quote by Mariame Kaba, “Let this radicalize you rather than lead you to despair.” After allowing myself time to get informed and feel my feelings, I looked for ways to get involved: donating to Texas abortion funds, amplifying messages from activists and community organizers on the ground in Texas, and vocalizing my support for abortion access.
BARCROFT MEDIAGETTY IMAGES
What personal or professional experiences have shaped the way you approach this work?
COURTESY
Cynthia Adriana Gutierrez, first-generation Nicaraguan Salvadoran and reproductive justice organizer: My personal experience of having an abortion at 22 years old has been at the forefront of how I approach this work. At the time of my abortion, I left an abusive relationship, was experiencing housing insecurity, lacked a steady income to support myself, and was living with a substance use disorder. Then, I learned I was pregnant. It was all too much to bear, and having an abortion was the best decision for me. I have no regrets and no shame around it. Being an abortion storyteller with We Testify, an organization meant to foster the leadership of people who had abortions, has transformed my work.
COURTESY
Chanel Porchia, founder of Ancient Song Doula Services: The stories of my grandmother having multiple miscarriages before having my mother, my sister having a child as a teenager and seeing how she was treated within her care, my own reproductive health experiences from my early 20s, into motherhood, and now into perimenopause. How was I made to feel in every instance of my care? Was it centered in informed consent? Did my grandmother have room to not feel shame when talking about her reproductive struggles? These questions were and continue to be foundational [for me] in centering the voices of others in their reproductive health choices.
PETE MAROVICHGETTY IMAGESADVERTISEMENT – CONTINUE READING BELOWhttps://d9e43064650e50b0be1c34272d9e7fb8.safeframe.googlesyndication.com/safeframe/1-0-38/html/container.html
The way we discuss reproductive rights and abortion access has long been debated. In what ways are we still failing to intentionally talk about this topic?
COURTESY
Ana Lucia Carmelo, MPH, healthcare consultant, public health advocate, and proud Peruvian immigrant: A major failure that comes to mind is the need to find a perfect victim. Folks really emphasized the fact that the Texas law would impact rape and incest victims, especially children. But why does support and empathy have to be conditional? I understand that part of it is to get folks who would not otherwise support abortions to see the worst case scenario of the law, but ultimately that perpetuates the stigma around abortions and makes folks continuously have to justify why they chose to have one. If we only agree with abortion in these worst case scenarios, we are saying that people only deserve bodily autonomy, empathy, and access to abortions once their bodies have been violated. We cannot be content with the bare minimum of legality without critically considering what care, empathy, and access look like for people who get an abortion.
If we only agree with abortion in these worst case scenarios, we are saying that people only deserve bodily autonomy, empathy, and access to abortions once their bodies have been violated.
COURTESY
Cynthia Adriana Gutierrez, first-generation Nicaraguan Salvadoran and reproductive justice organizer: When it comes to speaking on reproductive justice—the human rights framework centering people of color in ensuring we all are able to decide if, when, and how to grow families free from violence and coercion—and abortion access, we must always prioritize people with lived experiences. We are the experts of our own lives and are the most qualified to shut down false narratives. I hope the Court listens to us. It’s shameful that BIPOC women who have abortions are not prioritized in the national conversation. There needs to be a more intentional attempt to include the voices of abortion storytellers with disabilities, parents, those who are undocumented, and queer, trans, and gender non-conforming folks. RELATED STORYThe Whitewashing of Reproductive Justice
How do you see Black and Latina women specifically being erased from this national conversation yet again?
COURTESY
Chanel Porchia, founder of Ancient Song Doula Services: Through the intentional silencing of our voices due to a lack of uplifting community-based organizations that directly work with those most impacted. When policymakers, organizations, and others don’t center those most impacted, we already know that the agenda was never set in our favor, but rather continues to center privilege and access through the white gaze. Organizations like SisterWeb, Ancient Song, Mamatoto Village, Birthmark Doulas, Kindred Space LA and more have been working tirelessly to center their communities, and that directly comes from listening and meeting people where they are, not where we think they should be.
Black women and our Latinx sisters are no longer asking to be heard, and out of necessity, we are now formulating our own standards of care.
COURTESY
Angela Doyinsola Aina, MPH, co-founder and executive director of the Black Mamas Matter Alliance: Black and Latinx women have long been ignored, along with their reproductive rights advocacy work. The fact that there’s a long history of reproductive coercion, obstetric violence, and denial of quality care experienced by Black and Latinx women in the U.S. is a further injustice. Black women and our Latinx sisters are no longer asking to be heard, and out of necessity, we are now formulating our own standards of care. That is what the Black Mamas Matter Alliance is about. We have created a space and network that centers Black mamas’ rights to advocate, drive research, build power, and shift culture for Black maternal health, rights, and justice.
Ana Lucia Carmelo, MPH, healthcare consultant, public health advocate, and proud Peruvian immigrant: A lot of people currently live in places where Roe v. Wade exists merely in statute; an abortion is not an attainable reality for them due to costs, lack of nearby facilities, or poor quality care. The possibility of Roe v. Wade being overturned is concerning, especially for BIPOC, but legalizing abortion is only one piece of what it would mean to make abortion accessible and destigmatized. Putting meaning behind phrases like “abortion is healthcare” or “my body, my choice” rests on complete access to affordable, dignified, and empathic reproductive healthcare. There is so much about how healthcare works in this country that is related to who we are, what we look like, and where we live. In my own experience getting an abortion at Planned Parenthood, it became clear to me just how impersonal abortion care can be, even in a “progressive” city like New York: the metal detectors upon entering, the lack of Spanish translators, the shuttling back and forth between rooms with no explanation, the open concept recovery rooms with no privacy, the constant mispronunciation of my name. A hyper-focus on protecting Roe v. Wade without considering the consistent access and quality issues that exist disregards the lived experience of so many people who have had an abortion. We need to protect the right to abortion, yes, but we also need to ensure that abortions are humanized, dignified, and accessible to any person that wants one.
What is the most important or impactful thing we can do to shift the tide of abortion access? What or who needs to change?
COURTESY
Chanel Porchia, founder of Ancient Song Doula Services: The entire conversation needs to change to understand that reproductive healthcare access in the United States is an embarrassment, to say the least, and needs to be addressed on a systemic level. When we continue to separate the full spectrum of care that individuals need at certain points in their reproductive life, of course it is Black, brown, and Indigenous peoples who feel the burden. Black, brown, and Indigenous birthing people and those seeking reproductive health services access deserve to be seen, heard, and loved.
COURTESY
Ana Lucia Carmelo, MPH, healthcare consultant, public health advocate, and proud Peruvian immigrant: Collectively, I believe the single most important or impactful thing we can do to shift the tide of abortion access is to pass universal healthcare. Radically reimagining healthcare is such an important aspect of access. We have examples where a different world is possible: free COVID-19 vaccines for everyone, for instance. This is on policymakers, but we have seen that they have no impetus to make progress without pressure from us.
Reproductive healthcare access in the United States is an embarrassment, to say the least, and needs to be addressed on a systemic level.
COURTESY
Cynthia Adriana Gutierrez, first-generation Nicaraguan Salvadoran and reproductive justice organizer: There are so many ways you can get involved, such as driving people to their appointments, making sure they have gas money, helping out with childcare or translations, and offering your home to folks who are traveling for multi-day procedures. And of course, continue donating to Texas abortion funds: La Frontera Fund, Lilith Fund, Texas Equal Access Fund, West Fund. You can donate to all of them at once here.
After traveling over six hours from Houston, Judith, 33, chats with Dr. Rebecca Taub (right) before getting a surgical abortion as assistant Carissa Blethen (left) looks on at the Trust Women clinic in Oklahoma City. Judith suffers from Type 1 diabetes, and her partner, with whom she shares four kids, has kidney failure. “ I am sick. Why would I want to bring kids into this world?”Gabrielle Lurie/The Chronicle
OKLAHOMA CITY — Ianthe Davis ended her bartending shift at 4 a.m. one recent morning in Dallas. An hour later, a friend picked her up and drove her three hours up Interstate 35 to this capital city so she could get an abortion — a procedure that became almost impossible to obtain in her home state of Texas after a new law went into effect this month.
At a clinic in Oklahoma City, Davis was treated by another woman who was far from home, Dr. Rebecca Taub. The obstetrician and gynecologist travels once a month from her home in the East Bay to the small clinic, where she performs dozens of abortions over the course of two days.
After the procedure, Davis and her friend turned around and drove home. As a bartender, Davis said, “If I don’t work, I don’t make money.”
A Texas woman, an Oklahoma clinic and a California doctor: The scene offered a snapshot of the landscape under the Texas law that bans nearly all abortions after an embryonic heartbeat is detected — usually around six weeks — and makes no exceptions for rape, sexual abuse or incest.
The new law also enables private citizens to sue anyone who either performs an abortion or “aids and abets” one — and collect $10,000 plus their legal fees if they win the case. The law has narrow exceptions to protect the life of the mother or if continuing a pregnancy would cause “substantial and irreversible impairment of a major bodily function.”
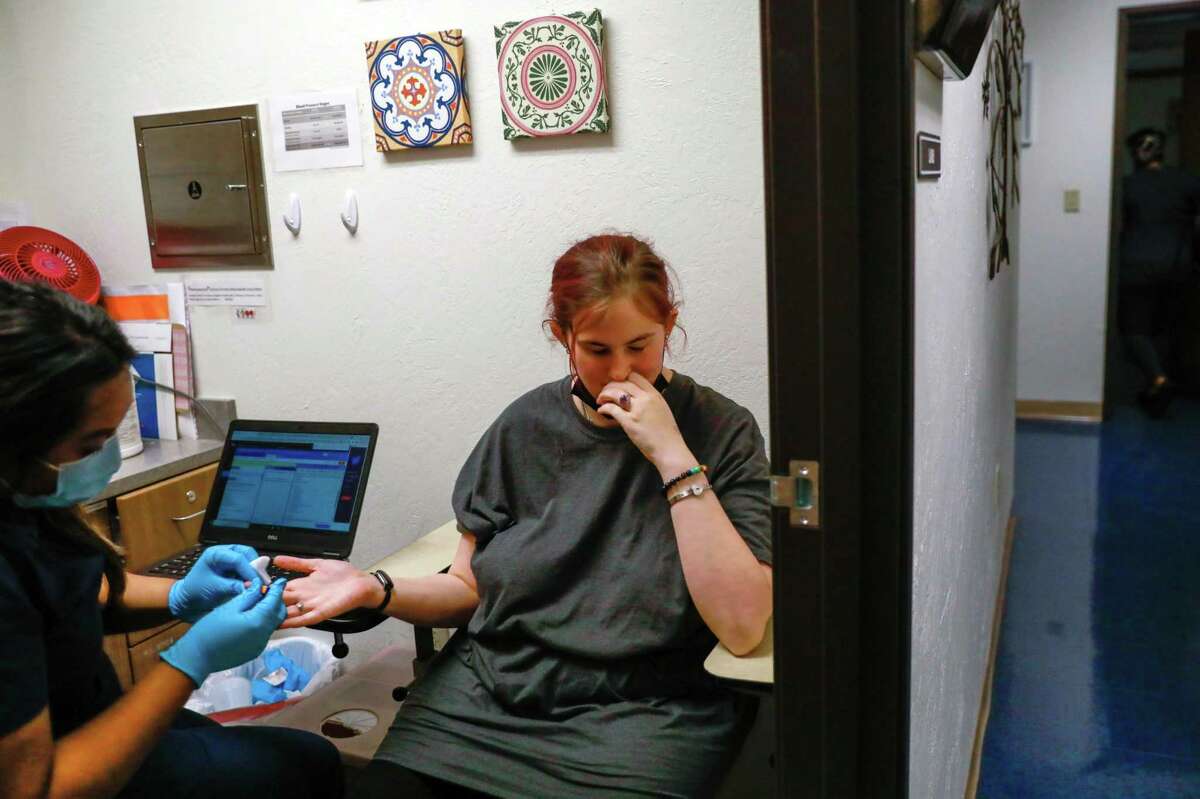
Ianthe Davis, 27, who traveled three hours from Dallas, lies still during an ultrasound at the Trust Women clinic in Oklahoma City. Davis was six weeks pregnant and unable to get an abortion in her home state, so she was forced to drive to Oklahoma.Gabrielle Lurie/The Chronicle
The Chronicle spoke to several women on a recent weekend who traveled from Texas to a one-story, mustard-brick building in suburban Oklahoma City called the Trust Women clinic, where Taub has been working.
Clinic officials said they have seen a roughly 50% increase in patients overall since the new legislation took effect, including 110 women from Texas over the past seven days. That is as many as visited the clinic during all of August.
The length of Davis’ journey is not unusual. Before the ban, the average woman of childbearing age in Texas lived 17 miles from the nearest abortion provider, according to the Guttmacher Institute, a research organization that supports abortion rights. Now, the average driving distance is 247 miles.
The Texans most affected by the new law will be women of color, who constitute 70% of those who received abortions in 2019, according to Guttmacher.
Abortion access is so limited in Dallas, the nation’s ninth-largest city, that Davis contacted a clinic there before the law took effect this month but was turned away. “They said they wouldn’t be able to” perform the procedure, she said. Demand for the clinic was so strong that she would have been 14 weeks pregnant by the time an appointment was available.
The new law confused Davis. She feared telling many people about her situation “because if you do, you might get charged or something like that. I know there are $10,000 rewards for people” who supply information about women obtaining abortions, she said.
She had heard of clinics in Arkansas and New Mexico that were seeing patients, but Trust Women was closer. When she arrived in Oklahoma City, she was just a few days over six weeks pregnant.
Dr. Rebecca Taub performs a surgical abortion at the Trust Women clinic in Oklahoma City. Taub, an OB-GYN specializing in family planning, travels once a month to the clinic in Oklahoma to perform both surgical and medical abortions.Gabrielle Lurie/The Chronicle
Davis said she understands placing limits on abortion. Roe vs. Wade, the 1973 Supreme Court ruling that provided women the right to have an abortion, permits the procedure until about 24 weeks, when the fetus can survive outside the womb.
“I do understand putting a limit, I get that part,” said Davis, 27. “Most people don’t find out because it’s like, soon as hell. And then there are people who were raped.”
Davis had a supportive family and a friend willing to drive her to a clinic. But she said she knows other Texas women who, because they can’t afford to travel out of state, are trying scientifically dubious methods of pregnancy termination that are popular online, like taking large amounts of vitamin C.
“But that just didn’t sound that effective to me,” she said. “So I made the drive.”
She worried about the extreme measures that others confronting unwanted pregnancies might attempt.
“It’s probably gonna get bad,” Davis said. “I mean, I heard one girl tried to drink bleach.”
The U.S. Justice Department sued the state of Texas to try to block the abortion law, saying it violates women’s constitutional rights by creating an “undue burden” on those who want to have an abortion. A hearing is scheduled for Oct. 1 in Texas.
Until then, a steady stream of women like Davis will continue coming to the Trust Women clinic, where they will be greeted by doctors like Taub.
Left: A poster on the wall of the locker room in the Trust Women clinic in Oklahoma City. Trust Women is one of the few clinics in Oklahoma to perform abortions. It is difficult for the clinic to find local doctors who will perform the procedure, so several physicians from other states make monthly trips there. Right: A stack of ultrasound images sits on a desk at the Trust Women clinic in Oklahoma City.Gabrielle Lurie/The Chronicle
The 35-year-old East Bay obstetrician and gynecologist, clad in blue surgical scrubs, performs roughly two dozen abortions a day when she is in town because it is difficult for the clinic to recruit local doctors, a common situation in states where the procedure is culturally shunned and women are required to scale many hurdles to obtain one.
To Taub, this is a form of activism. After seeing out-of-state patients and calls to the Oklahoma City clinic swell after the Texas law passed — two-thirds of the calls to the clinic inquiring about services are now from the neighboring state — she wants to do more.
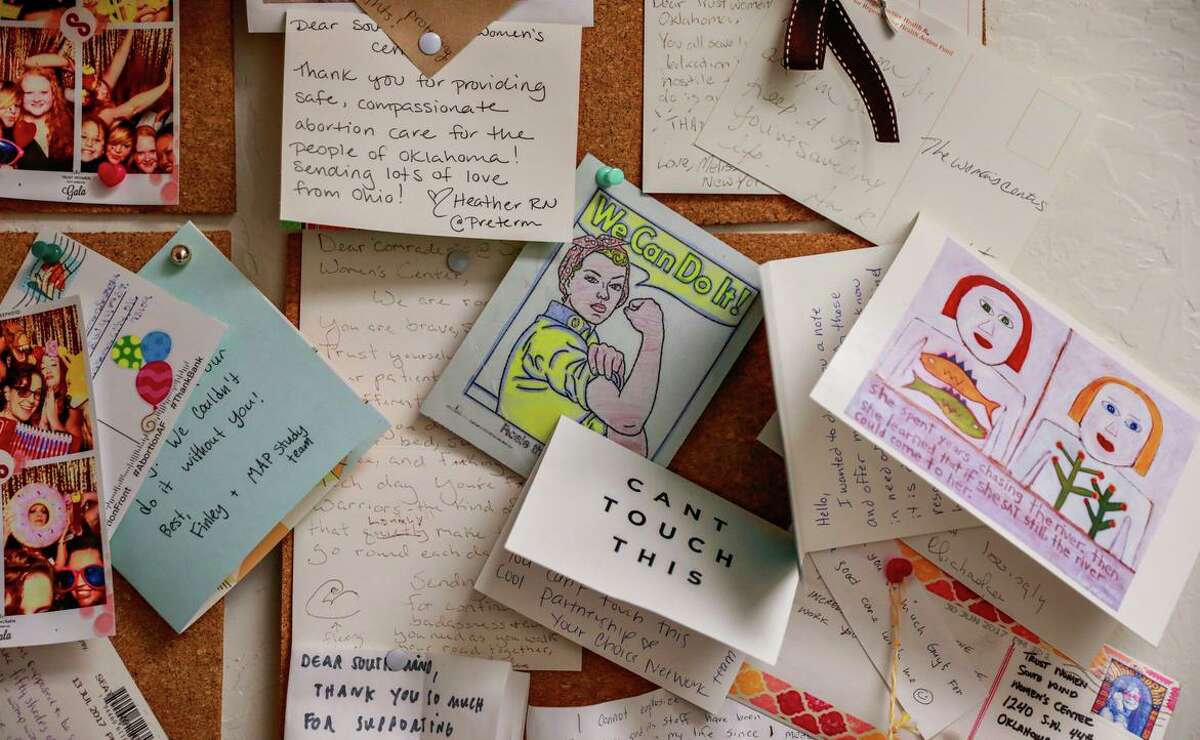
On this day, the waiting room was full of women seeking services they couldn’t find close to home. The clinic’s halls and waiting rooms were full of affirming messages, including posters saying, “We Love You!” “Everyone Loves Someone Who Had an Abortion” and “Prove Them Wrong.”
“There’s an urgency to the work that people who work with the clinic follow because they’re activists and they believe in this work,” Taub said. Since the Texas law took effect, her work “has definitely taken on a new urgency.”
The people who work at the clinic see the urgency in the faces of women like Daffnay McCoy. She, too, had an appointment for an abortion scheduled in Dallas. But she said that when the law took effect, clinic providers there explained that things had changed: They could give her a sonogram, they said, but wouldn’t perform an abortion.
After traveling three hours from Dallas, Daffany McCoy, 28, rests in the recovery room after getting a surgical abortion at the Trust Women clinic in Oklahoma City.Gabrielle Lurie/The Chronicle
“It kind of kind of freaked me out.” McCoy said. “I got hysterical and started panicking. I was hallucinating like I was going crazy.”
She said she has suffered from depression in the past and was worried that not being able to secure an abortion “was about to bring me back to that dark place.”
McCoy was already so stressed by her job in the payroll department for a Texas company, she said, that she had been suffering minor seizures. She has two children and felt she wouldn’t be able to adequately care for another. She said she is no longer with the father of her two children — who also impregnated her most recently — though he drove her to the clinic along with their children.
McCoy said she wouldn’t have known she was even pregnant if she hadn’t gone to the hospital because she was ill.
“But at that time, I was already past six weeks,” she said.
Thank-you notes are posted on the wall at the Trust Women clinic in Oklahoma City, one of the few clinics in Oklahoma to perform abortions. It is difficult for the clinic to find local doctors who will perform abortions, so several physicians make trips there from out of state.Gabrielle Lurie/The Chronicle
Once she arrived in Oklahoma City, wearing a T-shirt that said “Fierce and Fabulous,” she said she summoned an inner strength. She wished people who wrote the Texas law — or those who criticize women for having abortions — would be more empathetic toward women with unwanted pregnancies.
“You don’t know how this life came about. You don’t know if someone has been raped. Or if someone is going through an illness or a mental(ly unstable) state of mind. You just never know,” she said. “So to be on the safe side. I just feel as though no one should be obligated to make decisions for another individual. It just doesn’t make sense.”
Judith said she felt the same way. The 33-year-old nurse’s assistant, who asked that her last name not be used because she does not want her family to know about her abortion, was five weeks along when she learned she was pregnant — too far along to find a clinic that could accommodate her before the onset of the law’s time limits.
She left her home in Houston at 6:30 a.m. so she could arrive at the Oklahoma City clinic in time for her surgical procedure. She completed the 6½-hour drive alone, but said it “wasn’t bad. I prayed. And I listened to my gospel music.”
It was worth it, she said, because she didn’t feel healthy enough to have another child. She has diabetes, and her partner has kidney problems that will soon require dialysis. Plus, she already has four children.
“We both are sickly people. We’re just not well,” Judith said. “If anything happens to us, who’s gonna take care of our baby?”
Courtney, who also asked to be identified only by her first name, drove three hours to the clinic from a small town near Dallas. She was eight weeks pregnant.
After traveling more than three hours from Grandview, Texas, Courtney, 20, waits to obtain a medication abortion at the Trust Women clinic in Oklahoma City. Of visiting abortion clinics in Texas, she said “All of them said they wouldn’t do it because the heartbeat bill passed and saying that it was too risky. It was extremely stressful. The reason I’m actually getting an abortion is that I’m worried about what it would do for my mental health and my physical health and my relationship with the rest of my family. I recently found out I have seizures. When I got pregnant it started happening more and more. I’m scared that being pregnant while having seizures would end my life.”Gabrielle Lurie/The Chronicle
The 20-year-old’s reasons for seeking an abortion were both personal and medical. She feared that if her devoutly Catholic family learned she was pregnant and unmarried, “they would isolate me from the rest of the family. So going to term with this is not an option for me.”
She also has a medical condition that causes seizures, which had increased since she became pregnant. “And so with that I’m scared that being pregnant while having seizures could end my life,” she said.
She tried to find a clinic in Texas, but “all of them said that they wouldn’t do it because of the heartbeat bill,” she said.
Adding to her stress was a clutch of anti-abortion demonstrators beyond the 6-foot-high wooden picket stockade fence that surrounds the Oklahoma City clinic. As she walked inside, she said she heard them say, “You’re committing murder. You’re sinning. If you need money, or a prayer, we can help. Your baby can be put up for adoption.”
“I’m sitting there having to bite my tongue. Literally having to bite my tongue to keep from speaking,” she said. “My arms are shaking, my hands are shaking, not even able to ignore them, because my emotions were being stirred up.”
Trust Women clinic officials are expecting the flood of Texas women driving north to grow. They’re considering expanding their hours and adding staff, and are trying to recruit more doctors like Taub — even if they have to pay to fly them into town. On Nov. 1, a similar fetal heartbeat bill is scheduled to take effect in Oklahoma. Abortion rights organizations are attempting to block it.
Since the Texas ruling, Taub said some of her California colleagues have asked her about traveling to clinics like she does.
But she has more immediate concerns about her patients once they leave Oklahoma and drive home to Texas.
“There are so many unknowns in how this law can and will be enforced that I am concerned that pharmacists in Texas may not fill prescriptions that they know come from an abortion clinic, even though they are not the medications that are going to enact the abortion,” Taub said, referring to ibuprofen and anti-nausea medication she prescribes.
Her advice to patients before they head back to Texas: “I told them that they had to fill their prescriptions in Oklahoma.”
Volunteer Jennifer Goodner helps patient Judith, 33, in a wheelchair after a surgical abortion at the Trust Women clinic in Oklahoma City. Judith had to travel more than six hours from Houston to get the procedure. Judith suffers from Type 1 diabetes and her partner, with whom she shares four kids, suffers from kidney failure. “ I am sick. Why would I want to bring kids into this world? I know that if I’m gone no one can mother them like I do,” she said.Gabrielle Lurie/The Chronicle
For these groups, access to abortion has long been entangled in other structural and historical issues
Long before Texas’s Senate Bill 8 (S.B. 8) went into effect on Sept. 1, making it the most restrictive abortion ban in the country, abortion rights advocates, providers and funds have been trying to interpret what the measure could actually mean for them, especially its most unprecedented provision: Private citizens, even people who live outside the state, are empowered to sue anyone they think may have “aided or abetted” someone getting an abortion after six weeks — before most people know they’re pregnant.
Many believe that, for those trying to access abortion care, anyone within their support system — from the doctor who administers the procedure to the fund that pays for their fees, and even the person who drives them to the clinic — could be liable for a civil suit for $10,000 for each abortion.
“That vagueness is definitely on purpose to confuse people and deter them from accessing the resources that they need, including calling clinics or abortion funds for their services,” said Nancy Cárdenas Peña, Texas state director for policy and advocacy at the National Latina Institute for Reproductive Justice (Latina Institute).
Antiabortion groups have praised the law as progress for their movement. “To have a significant piece of pro-life legislation that takes effect when it was scheduled — that almost never happens,” John Seago, legislative director for Texas Right to Life, the antiabortion organization that helped draft the bill, told The Lily when the law went into effect. “It’s a phenomenal victory for our movement.”
While the right to an abortion is still protected by Roe v. Wade, abortion rights advocates fear that S.B. 8 will effectively isolate a pregnant person from receiving abortion care in Texas — eliminating abortion rights for 85 to 95 percent of all birthing people in the state, according to providers. What’s more, advocates say, people of color, who already experience higher rates of unintended pregnancy, higher maternal mortality rates, and unequal access to quality reproductive care and social services, will bear the burden of this law.
“Black womxn live in a state where there is already little to no support to provide care for any newly created family units,” said the Dallas-based Afiya Center in a statement. “[Temporary Assistance for Needy Families] and [the Supplemental Nutrition Assistance Program] are already overburdened and not fully funded for 100-percent participation. The [Child Protective Services] system is overloaded. Communal support is overextended. And lawmakers have decided that the best course of action is to make the ultimate decision on whether or not to have children.”
For Indigenous, immigrant and undocumented pregnant people, who represent some of the most marginalized groups in Texas, access to abortion is deeply entangled in other structural and historical issues. Many already experience some form of abortion prohibition, according to advocates, and S.B. 8 only serves to further cement this reality.
The main barrier to abortion access for these groups before S.B. 8 was financial, according to advocates. Since 2017, Texas law has forbidden insurers from covering abortion in both state-regulated and private plans (unless the patient is in danger of death or serious physical injury), leading pregnant people seeking the procedure to either purchase separate abortion insurance or pay out of pocket. Abortions typically cost between $300 and $800 for a medication abortion and between $300 and $1,500 for a surgical abortion, according to the American Civil Liberties Union of Texas — a burdensome fee for low-income pregnant people, especially considering additional costs, such as travel and child or elder care.
Some pregnant people are instead forced to carry unwanted pregnancies to term even when they can’t afford to. The annual cost to raise a child in this country is around $15,000. For those who cannot bear the expense — who are more likely to be people of color, given the country’s racial wage gap — it can trap them in a cycle of poverty.
Indigenous women and gender-nonconforming people have long been subjected to a de facto abortion ban, advocates say. Many Indigenous people cannot afford private health insurance, so they rely on the federal Indian Health Service (IHS), which serves as the main health-care provider to about 2.5 million American Indians and Alaska Natives. IHS was a provision born from treaties Native peoples entered into with the United States, for land seized. As a federal agency, it’s subject to the Hyde Amendment, which blocks federal funds from covering abortion services. That has historically made abortion for low-income pregnant people — especially people of color — a privilege, not a right.
“We’re the only race in the country that is denied access to abortion merely because of our race,” Charon Asetoyer (Comanche), founder and executive director of the Native American Women’s Health Education Resource Center on the Yankton Sioux reservation in South Dakota, told Indian Country Today. “We access health care through the federal government, and the federal government prohibits funds for abortion services.”
For Native women, limited access to abortion care can be devastating, advocates say. (According to 2012 Justice Department statistics, 1 in 3 Indigenous women is raped or is a victim of attempted rape.) Nearly half (46 percent) of Native women have their first child before age 20, and American Indian and Alaska Native women are 2½ times more likely to suffer a pregnancy-related death than White women.
“Indigenous peoples have been treated as if we don’t know how to manage our own land and families, thus having the government do it,” said Rachael Lorenzo (Mescalero Apache, Laguna Pueblo and Chicana), the abortion access lead at Indigenous Women Rising, via email.
Indigenous Women Rising is the only abortion fund in the country dedicated to assisting Native women and is culturally sensitive to their specific needs, according to Lorenzo. For example, many live in multigenerational households, where mothers are also caregivers of their parents or other elders, which, in Texas, could make it difficult for them to leave to access abortion services potentially hundreds of miles away. Indigenous women and queer people also suffer from extraordinarily high rates of violence, so the group is mindful of how and when it engages callers. “We are intimately familiar with the unique circumstances our community members are in,” said Lorenzo.
Abortion is not covered by Medicaid in Texas (unless in cases of rape, incest or life-threatening conditions — and S.B. 8 outlaws two of those three cases after six weeks of gestation), but it is in New Mexico, the only state neighboring Texas that doesn’t have a “heartbeat” law and where Indigenous Women Rising is based. That partly explains why most callers are from out of state, especially from conservative states, according to Lorenzo.
When S.B. 8 went into effect, the group anticipated an influx of calls from Indigenous people in Texas who would need abortion care, Lorenzo said: “We have spent the last week letting abortion funds and clinics nationwide know we are open and have funding to help.”
For low-income immigrants, accessing affordable health care can be extremely difficult. Most lawful permanent residents must wait a minimum of five years to be eligible for Medicaid, and that’s only if they meet all other eligibility criteria; in 2019, 25 percent of lawfully present immigrants and 46 percent of undocumented persons were uninsured, compared with 9 percent of U.S. citizens.
And while Medicaid does not cover abortion services because of the Hyde Amendment, it can be a crucial means of accessing contraceptives or other family planning services. Nearly half of uninsured Asian Americans are not citizens, and because undocumented community members are barred from Medicaid or buying insurance through the Affordable Care Act marketplace, those in financially vulnerable positions may have no other avenues to affordable health care.
“Immigrant women experience much higher rates of uninsurance than U.S.-born White Americans,” said Sung Yeon Choimorrow, executive director of the National Asian Pacific American Women’s Forum (NAPAWF), one of the only groups in Texas speaking to Asian American and Pacific Islander (AAPI) communities specifically about reproductive health, in an email. “Without insurance, contraceptives become expensive to afford.”
What’s more, language barriers present their own challenges. Community members with limited English proficiency are less likely to have a primary care doctor they see regularly or a usual place they go to for their health-care needs and emergencies, Choimorrow said.
“S.B. 8 will further isolate low-income and immigrant AAPI’s by putting abortions out of reach in terms of cost and accessibility,” she said.
There’s also the issue of documentation.
In Texas’s Rio Grande Valley, only one abortion clinic remains open today, to serve a population of more than 1 million. With S.B. 8, it’s a race against time for patients in the region to secure an appointment before the six-week mark. Many are anticipating to travel out of state for care (if they can afford the travel costs), but for those who are undocumented, travel can be risky; and for those in mixed-status families, who already have children, that risk may simply be too great.
“Transportation may seem as simple as going from point A to B, but that conversation is very different here in the Rio Grande Valley,” said the Latina Institute’s Cárdenas Peña.
Border wall funding has also meant increased militarization of the Valley, including increased surveillance, according to Cárdenas Peña. Not only are undocumented persons subjected to internal immigration checkpoints, but additional checkpoints are sometimes set up at random, which, Cárdenas Peña argued, has deterred people from going to their abortion care appointments.
“It isn’t only legislation around abortion access that affects someone’s access to abortion,” Cárdenas Peña said.
Tokyo 2020 Olympics – Basketball – Women – Gold medal match – United States v Japan – Saitama Super Arena, Saitama, Japan – August 8, 2021. Sue Bird of the United States and Diana Taurasi of the United States celebrate after winning the gold medal match against Japan REUTERS/Brian Snyder/File Photo
WASHINGTON, Sept 20 (Reuters) – A group of prominent women athletes including soccer star Megan Rapinoe and basketball standouts Diana Taurasi and Sue Bird on Monday urged the U.S. Supreme Court to protect abortion rights in a case involving Mississippi’s Republican-backed bid to ban the procedure after 15 weeks of pregnancy.
Abortion opponents have asked the court, which has a 6-3 conservative majority, to overturn the landmark 1973 Roe v. Wade ruling that recognized a woman’s right to end a pregnancy and made abortion legal nationwide after it was outlawed in certain states.
More than 500 athletes and groups signed a friend-of-the-court brief to the justices, including 26 Olympians, 73 professional athletes and various athlete associations. They argued that abortion rights have helped the growth of women’s sports and expressed concern that future athletes would suffer without those protections.
Without the right to terminate a pregnancy, “the physical tolls of forced pregnancy and childbirth would undermine athletes’ ability to actualize their full human potential,” the brief stated.
“As women athletes and people in sports, we must have the power to make important decisions about our own bodies and exert control over our reproductive lives,” Rapinoe, a two-time World Cup winner and an Olympic gold medalist, said in a statement, calling legislation curbing abortion rights “infuriating and un-American.”
Rapinoe has been outspoken on various political issues. Bird and Taurasi, both stars in the WNBA, helped the U.S. women’s basketball team win the gold medal at this year’s Tokyo Olympics. Taurasi is the WNBA’s all-time leading scorer. Bird is married to Rapinoe.
Other signatories included Ashleigh Johnson, the first Black woman on the U.S. Olympic water polo team and also an Olympic gold medalist in Tokyo.
The Supreme Court on Monday has set oral arguments in the case for Dec. 1. A ruling is due by the end of next June.
Mississippi Attorney General Lynn Fitch, a Republican backed by abortion opponents, said in papers filed with the court in July that the Roe v. Wade ruling and a subsequent 1992 decision that affirmed it were both “egregiously wrong” and should be overturned.
Mississippi’s court filing marked the first time that the Republican-governed state, in seeking to revive a law blocked by lower courts, made overturning Roe v. Wade a central part of its argument.
As party of an agenda to protect New Yorkers’ abortion access, Gov. Kathy Hochul urged Facebook to combat misinformation about abortion. Spencer Platt/Getty Images
“The rights of those who are seeking abortion services will always be protected here,” said New York Gov. Kathy Hochul in response to the Texas ban.
New York Gov. Kathy Hochul announced a plan last week to protect and expand abortion access for New Yorkers in response to Texas SB 8 and other anti-abortion laws across the country.
“Abortion access is safe in New York—the rights of those who are seeking abortion services will always be protected here,” Hochul said at a Monday press conference. “To the women of Texas, I want to say I am with you. Lady Liberty is here to welcome you with open arms.”
The agenda includes launching a public information campaign to address patient rights, ensuring easy access to telemedicine abortion, and urging Facebook to combat misinformation about abortion. Hochul wrote a letter to Facebook cofounder and CEO Mark Zuckerberg about the “rampant falsehoods and misinformation” on abortion and to urge the company to “take additional action to curb the spread of this misinformation.”
At the press conference last Monday, Hochul was joined by advocates and legislators including Sen. Kirsten Gillibrand, a longtime ally for abortion rights who stressed that these efforts need to come from the federal government too.
“The recent law in Texas—and the Supreme Court’s refusal to block it—is dangerous and disturbing. This law is not just unconscionable, it’s unconstitutional,” Gillibrand said. “At the federal level, we must pass the Women’s Health Protection Act, which would create federal protections against state restrictions that fail to protect women’s health and intrude upon personal decision-making.”
The House of Representatives is set to vote on the Women’s Health Protection Act this week. The bill was first introduced in 2013, but this will be the first vote on the legislation, which would prevent states from passing abortion restrictions like Texas SB 8.
Hochul was also joined at the press conference by Donna Lieberman, executive director of the New York Civil Liberties Union. “We’ve done it before and we’ll do it again: New York will open its doors to those in need of an abortion and stand up against any state that puts a bounty on reproductive freedom,” Lieberman said. “We will not let Texas, or any other state that tries to follow suit, turn back the clock.”
Just two weeks after the Supreme Court gutted Roe v. Wade, and with half the states in the country poised to follow in Texas’ footsteps and enact near-total abortion bans, Hochul’s announcement came not a minute too soon and should serve as a model for other states.
Gov. Hochul leads a press conference on abortion rights (photo: Don Pollard/Governor’s Office)
In response to the recent ban in Texas and upcoming Supreme Court case, Governor Kathy Hochul declared New York a safe harbor for abortion care at a rally on September 13. Hochul noted, rightly, that the state has an obligation to fully implement the 2019 Reproductive Health Act (RHA). To that end, she directed state agencies to launch public information campaigns directed at patients and providers about their rights and responsibilities under the RHA.
Senator Kirsten Gillibrand followed by voicing her support for the Women’s Health Protection Act, which would codify a right to abortion care into federal law, just as the RHA does in New York State.
These pronouncements of solidarity with people in Texas and other legally restrictive states are welcome first steps. As the right to safe, legal abortion nationwide hangs in the balance, however, reactive measures are no longer enough—if New York is to become a safe harbor for abortion, officials at every level of government must champion bold, proactive policies that pre-empt attacks from the powerful anti-abortion movement.
First, they must make abortion, and all forms of sexual and reproductive health care, accessible to all New Yorkers.
In 1994, SisterSong Women of Color Reproductive Justice Collective defined reproductive justice as “the human right to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.”
For decades, the fight for reproductive justice in City Hall and Albany has been relegated to a small handful of electeds and constituent activists. Access to abortion care isn’t simply a “women’s issue,” but City Hall and Albany continue to treat it as one. Marginalized New Yorkers, particularly the Black birthing people at the forefront of the reproductive justice movement whose communities are disproportionately affected by our collective inaction, know that abortion access is a social, economic, gender, and racial issue.
In New York City alone, there are at least 11 “crisis pregnancy centers,” which are fake health clinics that use lies and unauthorized medical practices to dissuade vulnerable birthing people from getting abortions. Anti-abortion extremists in Queens are now allowed, thanks to the 2nd U.S. Court of Appeals, to terrorize New Yorkers who try to access or provide reproductive health care in clinics.
While our city became the first in the nation to provide direct funding for abortion, the $250,000 that the City Council has set aside the last two budget cycles for the New York Abortion Access Fund isn’t nearly enough to cover the up-to-$3,000 cost of abortion care for low-income and uninsured New Yorkers, let alone out-of-state birthing people.
These are some of the many hurdles New Yorkers face in accessing abortion care, and abortion care is only one piece of the larger problem. Systemic racism in health care for pregnant and birthing New Yorkers, inadequate postpartum care and early childcare, stigmatizing, outdated sex-ed, the proliferation of gender-based and sexual violence—we could go on—are just some of the others. In the spirit of reproductive justice, we cannot talk about shoring up abortion access in New York without also talking about the persisting inequities in all facets of sexual and reproductive health care.
Now that we face an impending national crisis, one that many marginalized communities have already been facing for years, New Yorkers are looking for ways to join the fight. Using our collective experience, knowledge, and skill sets, we’ve put together a non-comprehensive action guide that outlines steps New York elected and government officials can take, at every level and in almost all offices, to truly make New York a safe harbor for abortion care.
The guide also includes graphics and call transcripts that everyday New Yorkers can use in their activism.
Finally, it’s past time for New Yorkers to elect more reproductive justice advocates to office.
The anti-abortion movement has spent millions to help elect extremists who champion their cause in state legislatures and city governments across the country. Yes, greater gender representation, as seen in our first woman Governor, and New York City’s first women-majority City Council come January, could result in more substantive gender representation in New York politics as well. But simply electing more women to power doesn’t necessarily ensure those political leaders will focus on reproductive justice. As it stands, champions of reproductive justice are still largely on the outskirts of political power.
The country faces the biggest threat to Roe v. Wade in decades. It’s incumbent on New York to set the example for other progressive cities and states that could face an influx of out-of-state patients seeking abortion care. We must elect candidates to office who are committed to making that possible. If we succeed, we can show purple and red cities and states, particularly those on the verge of securing Democratic wins in their legislative or executive offices, that reproductive justice advocates can run and win.
*** Astrid Aune is a community organizer and 1L at CUNY School of Law. Elizabeth Adams is a Legislative Director at the New York City Council, formerly served as the Director of Government Relations at Planned Parenthood of NYC and was a candidate for City Council in Brooklyn’s 33rd District. Jessica Madris is a freelance reporter and writer covering gender policy, particularly at the local level, with an MPA in Urban Social Policy and Gender and Public Policy and experience in city government and politics, and a postpartum doula in Brooklyn.