Demonstrators in favour of legalising abortion react after the Senate passed an abortion bill, in Buenos Aires, Argentina on December 30, 2020 [File: Reuters/Agustin Marcarian]
The Argentinian government must continue to dismantle barriers women face in accessing safe abortion.
In recent months, Argentinians have had access to legal abortion for the first time. In December, Argentina became the fourth in Latin America to legalise abortion after the National Congress passed the Voluntary Termination of Pregnancy Law
Securing this right for women and pregnant persons was a milestone achievement and the culmination of decades of struggle, setbacks and progress. Now, new challenges emerge: the effective implementation of the law across a vast and unequal territory and the legal battles filed by conservative groups in the nation’s courts.
Amnesty International is currently monitoring the enforcement of the Voluntary Termination of Pregnancy Law. We have examined at least 33 lawsuits that challenged the law, 20 of which have already been dismissed – at least three of these dismissals are final.
So far, none of the suits filed against the Argentine state claiming that the law is unconstitutional has been successful. Despite some judges being willing to put their religious or personal interests before the rights of women and pregnant persons, in general terms, the judiciary has shown itself to be a guarantor of human rights and, hopefully, it will continue to resist the attacks that attempt to overturn a law approved by a vast majority of Argentina’s Congress.
An additional challenge faced by citizens who want to access this service is that Argentina is a federal state in which each of the 24 jurisdictional authorities is free to determine their own health policies. There are also wide economic and social inequality gaps between the provinces, varying levels of ecclesiastical influence and marked ideological differences between federal governments. These factors all impact the effectiveness of the implementation of the Voluntary Termination of Pregnancy law.
In many rural areas, sexual and reproductive health services and trained staff are still unavailable. The province of Catamarca, for example, is home to more than 124,000 women and people of childbearing capacity, according to the National Institute of Statistics and Censuses, but, in a response to a freedom of information request by Amnesty International Argentina, the Ministry of Health in Catamarca revealed the region only has two healthcare centres that guarantee access to services for the voluntary termination of a pregnancy.
The province of Buenos Aires, home to 40 percent of the national population, has made significant progress, yet 36 of its 135 districts still do not offer this service. As this is a national law, anyone should be able to get an abortion no later than 10 days after they request it, irrespective of their place of residence. Delays or obstructions represent a violation to their rights.
Access to information is also key to making free decisions. The government has still not organised massive information campaigns to help people know their rights and the options available to them when deciding to terminate a pregnancy.
It is also necessary to have quality nationwide statistical data to have diagnostic tools in connection with the progress and the challenges in the implementation of the law at a federal level. It is also essential to guarantee that students have access to comprehensive sex education, a policy that is experiencing some obstructions in certain jurisdictions.
Abortion access procedures have presented some issues that need to be overcome. The authorities must approve the production and sale of mifepristone, a drug recommended by the World Health Organization, which has been on the list of essential medicines since 2005. This drug, combined with misoprostol, boosts the efficacy of pregnancy terminations and speeds up the process.
Likewise, it is essential to improve the accessibility to interventions using manual vacuum aspiration (MVA), since almost all provinces continue to perform curettage, a less safe method that should be reserved only for those cases where other options are not available.
The women’s rights movement has a lot to celebrate. Argentina has brought abortions out of clandestine settings thanks to activism, research and vital public debates. This same path continues to inspire activists across the region, who also seek sexual and reproductive autonomy. The green wave keeps spreading across Latin America and will surely bring new victories in the recognition of women’s rights.
Attorney Michelle Simpson Tuegel is asking for a ruling against Gov. Greg Abbott, Attorney General Ken Paxton, and the Republican lawmakers who backed SB 8, alleging they didn’t have the authority to pass the law. Robert Daemmrich Photography Inc/Corbis via Getty Images
A Dallas attorney is suing Texas Right to Life to stop it from filing future lawsuits against her. It’s an unusual move, but SB 8 is an unusual law.
In one week, the most extreme—and, frankly, bonkers—abortion ban will go into effect in Texas.
Much has been written about the absurd nature of Senate Bill 8: Texas Republicans banned abortion at six weeks’ gestation, which is before many people know they’re pregnant. Even worse than that, however, they’ve turned enforcement of the law over to the public.
SB 8 deputizes anyone in the country to become an abortion enforcer in Texas: If you suspect that a person has provided an abortion, aided and abetted an abortion, or merely intends to do either of those things in violation of SB 8, then you can sue that person! And if you win, you’ll collect at least $10,000—maybe more!
It’s nice work if you can get it.
And Texas Right to Life (TRL) is trying to get it. But not if Michelle Simpson Tuegel—an attorney and victims’ rights advocate in Dallas, who famously won a settlement for the gymnasts abused by longtime USA Gymnastics team coach Larry Nassar—has anything to say about it.
Earlier this week, Tuegel filed a lawsuit seeking a temporary restraining order against Texas Right to Life and its legislative director, John Seago, barring them from filing lawsuits against her under SB 8. (She is also asking for a ruling against Gov. Greg Abbott, Attorney General Ken Paxton, and the Republican lawmakers who backed SB 8, alleging they didn’t have the authority to pass the law. She says the law violates her rights under the U.S. and Texas constitutions.)
Suing TRL to stop the organization from filing future lawsuits against her is an unusual move, to be sure. But SB 8 is an unusual law.
Under normal circumstances, Tuegel would have filed a lawsuit against Greg Abbott and Ken Paxton and asked the court to enjoin government officials from enforcing SB 8. The court would have likely granted the restraining order because SB 8 is a pre-viability abortion ban and—sing it with me—pre-viability abortion bans are unconstitutional.
But Texas is tired of hearing that refrain. For nearly a decade—since the explosion of abortion restrictions in 2011—Texas has been leading the way at throwing abortion bans at the wall to see which ones will stick. And for nearly a decade, courts have been slapping Texas in the face and telling Texas to knock it off.
So to get around this pesky problem of courts striking down their blatantly unconstitutional laws, Texas Republicans crafted a law that makes it virtually impossible to successfully challenge.
SB 8 turns over enforcement of the law to private citizens and forbids its enforcement by public officials.
This way, anyone wanting to challenge the law literally can’t. They can’t file a lawsuit against the attorney general or the head of the department of health—the traditional defendants in lawsuits like these—because public officials have no enforcement power. You can’t sue a public official for something they will never do, and which the law says they’re not allowed to do.
But that doesn’t mean Tuegel isn’t going to give it a go.
SB 8 creates a ‘mercenary society’ rife with chaos
SB 8 is a “gross and obvious legislative overreach,” according to the lawsuit, and it “creates a mercenary society” by deputizing private citizens to enforce the law and allowing everyone except government officials to bring a civil lawsuit against people who violate the law.
And who are those people? Anyone who provides an abortion in violation of the law, aids and abets such an abortion (whatever that means), or even simply intends to do those things.
“SB 8 places a bounty on people who provide, aid, speak about, or indeed, even think about abortions, inviting random strangers to sue them throughout the state,” Tuegel’s lawsuit says.
Tuegel claims the law is unconstitutionally vague; it doesn’t specify what aiding and abetting is. Does driving someone to a clinic count? What if you walk into a clinic to use their bathroom because you really have to pee, and you see a pregnant woman coming up behind you so, being the kind person you are, you stop and hold the door for them? Well, my friend, you may have just aided and abetted an abortion, and you may be liable. Or you may not be. That’s the thing. No one knows because the law is a disaster.The law is a cynical effort to drive abortion rights out of the courtroom and under the control of mercenaries: rogue agents like Texas Right to Life who are accepting “tips” from God-knows-where alleging God-knows-what against God-knows-whom.
The preparation for September 1, when the law goes into effect, has been hilariously disastrous: Last week, a website popped up encouraging enforcement and reporting of people that could be sued for violating SB 8. You can “join the Team of Pro-Lifers working to enforce the Texas Heartbeat Act,” according to the website hosted by TRL. (This past weekend, the website was flooded with fake tips from individuals claiming to work at abortion clinics: My favorite tip from a list of options posted on social media was, “I saw the receptionist throw nail polish at an elderly man,” which somehow captures the absurdity of this entire affair.) In response to this deluge, TRL seems to have begun blocking IP addresses from outside Texas … as if virtual private networks (VPNs) don’t exist.
Undeterred by the procedural cesspool Texas Republicans have created, Tuegel isn’t just asking for injunctive relief against Texas Right to Life and John Seago. She’s also seeking declaratory relief against Abbott, Paxton, and every state senator and representative who sponsored the law. (Declaratory relief is when a litigant goes into court not seeking monetary damages, but just wanting to understand what their rights are.)
In this case, Tuegel wants to know whether the law violates a host of rights under both the Texas and U.S. constitutions, including her right to free speech (because talking about abortion with a client who then proceeds to get an abortion could open her up to civil liability) and her right under the Texas constitution to have her day in court.
Setting aside the important First Amendment rights at issue in this case—rights which conservative Republicans generally pretend to care about, but perhaps only when it involves sanctioning the refusal to bake cakes for gay couples—the law is a cynical effort to drive abortion rights out of the courtroom and under the control of mercenaries: rogue agents like TRL who are accepting “tips” from God-knows-where alleging God-knows-what against God-knows-whom.
SB 8 penalizes attorneys for challenging Texas’ unconstitutional abortion restrictions
The Texas Constitution contains an “open courts” provision that guarantees all litigants the right to redress their grievances and the right to have their day in court. But SB 8 makes this virtually impossible in a way that is damn near diabolical.
To understand how, I’m going to have to talk to you about attorneys’ fees and lawsuit costs, so strap in.
Lawsuits are expensive and can take years to resolve. When Texas lost Whole Woman’s Health v. Hellerstedt, Texas taxpayers took a hit to the tune of $3.6 million. The costs of filing court documents, conducting discovery, and going through the trial and appeals process costs hundreds of thousands of dollars—millions if the case makes it to the Supreme Court. These fees often act as a deterrent: Courts will sometimes order the losing party to pay the prevailing party’s costs and attorneys’ fees. If you don’t have a good case, you could end up owing an alarming amount of money. That’s a daunting prospect for a group of abortion snitches like Texas Right to Life. So Texas Republicans put their thumb on the scale.
The Texas law intentionally drives a wedge between attorneys and their clients when it comes to abortion rights litigation. Any attorney who challenges an abortion restriction in Texas and loses any of their claims automatically becomes liable for the other side’s attorneys’ fees along with their client. That means if their client can’t pay, the attorney will have to cough up the money.
Any attorney who decides to represent a target of these abortion snitches risks their entire business by bringing a claim challenging the constitutionality of Texas’ abortion laws.
I cannot overstate how unusual this is. When a party to a lawsuit is the prevailing party in that lawsuit, if the law permits them to recoup attorneys’ fees from the other side, usually that burden falls solely on the litigant and not the litigant’s attorney.
And this doesn’t apply only when attorneys challenge SB 8. It applies when attorneys challenge any of the dozen abortion restrictions that Texas has on the books. It fundamentally changes the way lawsuits operate procedurally.
But it gets worse: The law also fiddles with the definition of “prevailing party” and further stacks the decks against attorneys challenging Texas’ abortion restrictions.
Usually a party to a lawsuit is deemed “the prevailing party” if they win their most important claims. Under Texas law, the prevailing party is the party “vindicated by the judgment rendered.”
But SB 8 changes that for abortion rights litigation. If you challenge an abortion law in Texas, you have to win every single claim you bring. If you don’t, the law says that you’re the losing party and you automatically become liable—with your client—for the other party’s attorneys’ fees.
So if you’re an attorney like Michelle Simpson Tuegel, and you challenge an abortion restriction (not just this six-week ban, but any restriction at all) you either must prevail on every single claim you bring or risk having to pay, whether in full or not, the other side’s costs.
If your first thought is, “what attorney is going to risk having to pay hundreds of thousands of dollars in attorneys’ fees to defend their clients from frivolous lawsuits brought by abortion snitches?” then congratulations! You’ve had the correct thought.
Michelle Simpson Tuegel says she will continue to counsel her clients about abortion even though she risks her entire law practice by doing so. But not many attorneys are willing to do that, which means a lot of people ensnared by this law won’t be able to find an attorney to represent them.
And that’s precisely what Texas Republicans intended.
The science is clear: abortion by medication is safe and effective
The pandemic has shown us that it’s time to change the way we get health care and that essential health care, including abortion, has always been out of reach for far too many. As we look ahead to the future of care, the science is clear: medication abortion care is safe and effective, and it’s past time to remove the restrictions on it. Now, actions from the FDA and new research show us that removing the restrictions on medication abortion care has the potential to expand access for many people who need care. The July 2021 special issue of the journal Contraception focuses on the restrictions on medication abortion, mifepristone, including its impacts on safety and efficacy, access to abortion, and burdens on patients and providers.
Mifepristone is regulated by a Risk Evaluation and Mitigation Strategy (REMS). REMS programs are rare and intended for drugs with a risk of very serious side effects. The mifepristone REMS includes three “Elements to Assure Safe Use”: mifepristone must be dispensed from a clinic, medical office or hospital (not a retail pharmacy); providers must register as certified prescribers; and patients must sign a patient agreement in addition to standard informed-consent forms. Together, these restrictions create a sense that mifepristone is dangerous for patients to use and overly complicated for health care providers to offer.
Massive quantities of data collected during the first 20 years of mifepristone’s use in the U.S. demonstrate that it is highly effective and exceedingly safe. Prior to 2020, opponents of loosening regulations on mifepristone could argue that mifepristone was safe for the nearly four million individuals who had used it in the U.S. because of the regulations. However, experience during the COVID-19 pandemic demonstrates that restrictions are not what make mifepristone safe.
During much of the pandemic, the in-person dispensing requirement for mifepristone was lifted in order to limit face-to-face contact. This meant that providers could send mifepristone through the mail to their patients following a telehealth evaluation. Patients received the counseling and care they needed, health care providers collected the necessary information to determine if mifepristone was an appropriate option, and both avoided the risk of contracting COVID-19. This change provided an opportunity to study how removing this requirement affected—or did not affect—the safety and efficacy of medication abortion care.
Twoarticles in the Contraception special issue describe medication abortion care in the U.S. provided through different protocols, including a telehealth visit followed by mailed medications; both find that these models of care are safe (less than 1 percent of patients experienced a serious complication) and effective (about 95 percent had a successful abortion without a follow-up procedure). Studies from the U.K. (52,142 patients in England and Wales and 663 patients in Scotland) reinforce that provision of medication abortion care via telehealth and mailed medications is safe, effective and highly acceptable to patients. Taken together, these recent studies reflect findings from the pre-COVID-19 era, reinforcing what we already knew: mifepristone is safe and effective, regardless of how and where it is dispensed.
Medically unnecessary restrictions impact health care providers’ ability to offer medication abortion care. A survey found that 24 percent of obstetrician-gynecologists not currently providing medication abortion care would do so if the in-person dispensing requirement were removed, potentially more than doubling the number of providers in the Southeast and Midwest, where abortion access is highly restricted. Many patients would prefer to receive abortion care from their primary care provider with whom they have a long-term relationship, but the REMS stands in the way.
Although medication abortion care is well within the scope of primary care, the REMS contributes to stigma and barriers at the individual and institutional level. Logistical challenges presented by the REMS (including the in-person dispensing requirement) and resistance from institutional decision-makers result in barriers for providers and unnecessary burdens for patients. Removing the REMS and allowing pharmacy dispensing of mifepristone could help normalize medication abortion care, facilitate provision in primary care and address disparities in abortion access.
Patients’ reasons for choosing telemedicine abortion with mailed medications highlight why this option is vitally important: patients describe the importance of privacy, protection from stigma, avoiding unnecessary contacts (particularly important during COVID) and travel. In an interview study of 45 patients in Hawaii, 13 percent said that they would have had to continue the pregnancy without the telehealth–mailed medication option. The ability to receive abortion care through telehealth is extremely important for improving access: providers can reach geographically distant patients, and one provider can serve an entire state without patients needing to find time, childcare and funds to travel.
With every passing year since the approval of mifepristone in 2000, research documenting its safety and efficacy grows, and each study reinforces and builds upon the last. We have more than enough high-quality data to support reconsidering how mifepristone is regulated and to remove the REMS. Doing so will not be a panacea for abortion access, given the complex web of abortion restrictions that many states impose, but it’s a necessary step towards bringing medication abortion care into line with the science. It’s time.
This is an opinion and analysis article; the views expressed by the author or authors are not necessarily those of Scientific American.
Congresswoman Carolyn B. Maloney, Chairwoman of the Committee on Oversight and Reform, speaks in Union Square on August 18, 2020 in New York.Bryan R. Smith / AFP via Getty Images
The dispensing rule is “not scientifically based or needed” and limits access to the drug, ob-gyn group official says.
A group of Democrats on the House Oversight Committee announced a resolution Thursday pressuring the Food and Drug Administration to permanently lift the in-person requirements on medication abortion, as the agency is evaluating its rules on abortion pills.
The resolution — backed by Chairwoman Carolyn Maloney of New York, Rep. Diana DeGette of Colorado, Rep. Barbara Lee of California, and Rep. Ayanna Pressley of Massachusetts — calls for policies related to medication abortion to be “grounded in science” and “ensure equitable access for patients.”
The resolution, first obtained by NBC News, says that lifting the in-person dispensing requirement and other restrictions for mifepristone would improve access without weakening the drug’s strong safety profile.
The FDA requires mifepristone, one of the two pills used in early pregnancy abortion, to be distributed in clinics or doctors’ offices rather than prescribed and picked up at pharmacies or by mail. In May, the Biden administration announced it would review those requirements for the drug.
However, in light of the coronavirus pandemic, a group of doctors and advocates, led by the American College of Obstetricians and Gynecologists, challenged the rule so that pregnant people could order the pills by mail. The agency temporarily eliminated the requirements on mifepristone first in July 2020, in response to a court order that was later reversed by the Supreme Court, and again in April.
“It’s time that we trust the science and ensure access to safe, legal abortion, particularly for communities where abortion care has been historically pushed out of reach,” Maloney said. “I plan to continue this fight until everyone can freely exercise their right to access abortion — including medication abortion.”
When medication abortion, which is the most common method in the first 10 weeks of pregnancy, is obtained by telemedicine or in person, the likelihood of complications is less than 1 percent, according to ACOG.
Jennifer Villavicencio, an ob-gyn and lead for equity transformation at ACOG, said the in-person dispensing requirement for the drug is “not scientifically based or needed” and creates a “barrier for people to access this medication in a political environment where it is already very difficult to obtain an abortion.”
Lee echoed the ACOG’s calls to eliminate the rules on abortion pills permanently.
“For people already experiencing health disparities — including people of color, people with lower incomes, and people in rural communities — the FDA’s restrictions often push access to medication abortion out of reach,” Lee said. “We cannot allow discriminatory stigma to keep people from accessing the health care they deserve.”
Texas school districts have been defying Gov. Greg Abbott by issuing mask mandates. Brandon Bell/Getty Images
As Texas Republicans decry mask mandates as infringing on their bodily autonomy, they keep stripping pregnant people of the right to bodily autonomy.
In Texas, all hell is breaking loose. First up: mask mandates.
In July, Texas Gov. Greg Abbott used an executive order to institute a ban on mask mandates by any government entity, including school districts. This is less than ideal, considering Texas has alarming COVID-19 rates and a dwindling number of ICU beds.
Plenty of local school districts issued mask mandates anyway. And at least one North Texas school district came up with a creative loophole: putting masks in the dress code. The Paris Independent School District, which covers around 4,000 students, said including mask wearing in the dress code was “consistent with its statutory authority.”
But the counties and school districts that defied Abbott more explicitly have been stuck in a legal battle with the state. They finally received some good news on Thursday, when the Texas Supreme Court ruled in their favor and refused to block temporary restraining orders against Abbott’s mask mandate ban. And a few hours later, the Texas Education Agency agreed to stop enforcing Abbott’s ban in the school systems while the legal fight is still ongoing.
If all that wasn’t bad enough, we haven’t even gotten to what’s going on with abortion in Texas.
Last Wednesday the Fifth Circuit Court of Appeals upheld a Texas law that effectively bans abortion at 15 weeks. This is five-alarm bad. It’s the first time a federal court has ever upheld a gestational ban.
This comes a couple of months after Abbott signed an even more draconian abortion ban: SB 8, which bans abortion at six weeks. The law has been challenged by abortion providers, and as we wait for a ruling from the district court as to whether it can go into effect on September 1, here are a few things to consider:
Banning abortion at six weeks is banning abortion. Period. Six weeks is before many people know they’re pregnant—and politicians like Abbott know this. That’s also why these laws are never upheld by the courts.
SB 8 also changes who has standing to sue abortion providers. In non-legalese: Typically you’ve got to have some skin in the game to sue someone. So in this case, you would have to be a patient. SB 8 changes that and grants standing to anyone. That means your racist uncle can sue an abortion provider or anyone involved in obtaining an abortion, like an abortion fund or the person who drives you to the clinic—essentially putting a bounty on them.
The Fifth Circuit decision indicates a judicial willingness to uphold bans that even a few years ago the court would have never considered. Even if the district court doesn’t let SB 8 go into effect, Texas will likely file an emergency appeal using the Fifth Circuit decision to effectively say, “Hey, you folks said we could implement a gestational ban!”
And did we mention that last week Brownsboro became the 15th East Texas community to ban abortion within city limits? Oh, and the Texas legislature is also advancing a bill restricting medication abortion access.
So what does this all mean? The TLDR is … quite honestly, not good. It means abortion access is dwindling in Texas, and there’s a real possibility that soon there truly won’t be any access to abortion in the state. This increasingly volatile landscape means that many Texans are already unsure if abortion is legal in their state.
The irony is not lost on us that as state Republicans decry mask mandates as infringing on their bodily autonomy, they’re stripping pregnant people of their rights to bodily autonomy.
But like abortion bans, mask mandate bans don’t actually have anything to do with public health. They’re both power grabs—policies put in place to further marginalize the vulnerable and keep the powerful in power.
Mississippi will no doubt use the Texas case to argue before Justice Amy Coney Barrett and the rest of the Supreme Court that it should uphold the state’s 15-week ban. Tom Williams-Pool/Getty Images
The Fifth Circuit’s decision to uphold a Texas ban on a common abortion method is a big deal.
Bad news out of the federal courts: On Wednesday, the Fifth Circuit Court of Appeals upheld a Texas ban on the method of abortion most commonly used after 15 weeks’ gestation: dilation and evacuation (D&E).
The Texas law is effectively a 15-week pre-viability abortion ban. And you know what we say about those kinds of bans: They’re unconstitutional! But the Fifth Circuit ignored the Constitution and upheld the Texas law anyway.
“Texas has been hellbent on legislating abortion out of existence, and it is galling that a federal court would uphold a law that so clearly defies decades of Supreme Court precedent,” Nancy Northup, president and CEO of the Center for Reproductive Rights, said in a statement.
In a rambling 109-page opinion that used inflammatory and misleading language, including the term “live dismemberment” to describe a D&E, the court upheld a law that would send doctors to prison for up to two years.
“This ban is about cutting off abortion access. … In no other area of medicine would politicians consider preventing docs from using a standard procedure. It should never be a crime for doctors to use their best medical judgment,” said Amy Hagstrom Miller, founder and CEO of Whole Woman’s Health, a plaintiff in the case.
This decision is a huge deal, as it’s the first time a federal court of appeals has upheld a pre-viability abortion ban. Ever. That means the law around abortion rights and access is already changing in real time.
The Supreme Court is the only court that can undo this decision now.
Speaking of the Supreme Court, all eyes are on the Court, which will hear the most consequential abortion case since Roe v. Wade next term. That case happens to involve—wait for it—a 15-week ban similar to the law just upheld.
It’s important to remember that Trump and other conservatives not only created an anti-abortion supermajority on the Supreme Court, but they stacked the lower courts too.
In fact, six judges on the Fifth Circuit are Trump judges.
Just last year, a three-judge panel of the Fifth Circuit struck down the exact same ban. But the other judges didn’t like that, so they decided on their own to rehear the case. This highly unusual move was a big red flag for abortion rights. The legal landscape is not the same as it was last year, and for abortion, it’s markedly worse.
This case proves that conservative judges are no longer waiting around for a Supreme Court decision to start gutting abortion access—they’re going to start chipping away at access with the power they already have. And it’s a lot of power!
Wednesday’s decision is the first time a federal court upheld a ban on gestational limitations. In a sort of chain reaction from hell, this will undoubtedly open the doors for other challenges to gestational limits in other states—including, most critically, Mississippi.
Mississippi will no doubt use this case to argue in Dobbs v. Jackson’s Women’s Health that the Supreme Court should uphold the state’s 15-week ban.
It could immediately impact access in Louisiana, which also has a 15-week abortion ban just waiting to be enforced if the Supreme Court lets the Mississippi law stand. The dominoes have started to fall.
Typically, when it comes to these types of cases, precedent controls. It means that judges don’t like to be the first to radically change the legal landscape on an issue. But that dynamic is shifting, and judges are getting bolder in their anti-abortion rulings.
An appeals court is upholding a ban on a common second-trimester procedure
The 5th Circuit Court of Appeals has upheld a Texas law banning dilation and evacuation abortion (D&E) after the first 15 weeks of pregnancy, the first federal court in the nation to do so. The move comes after a federal court deemed the ban unconstitutional just last year—the reversal effectively targets the most common method of abortion used in second-trimester pregnancies.
Doctors who violate the ban will face up to two years in prison.
The law was first passed in 2017, but was blocked by court battles. A federal judge in the lower courts had previously invoked the “undue burden” test, ruling that the law would amount “to a ban on all D&E abortions.” But on Wednesday, the appeals court argued that doctors could still perform the procedure while complying with the legislation—which requires doctors to first stop the fetus’s heart by inserting a large needle into the abdomen or cervix—handing the anti-abortion movement a victory.
The ruling is just one of many looming crises for abortion access in Texas. S.B. 8, which bans abortion after six weeks of pregnancy—before many people even know they’re pregnant—is scheduled to go into effect on September 1. According to Planned Parenthood, the law would also allow anyone to “sue doctors and others who help a Texan access abortion in the state.” This effectively turns anyone with an agenda into a bounty hunter for people who get abortions and those who perform them.
These laws are just another way for anti-abortion lawmakers and activists to challenge Roe v. Wade, chipping away at abortion rights little by little without explicitly outlawing abortion. (Though the effect can be virtually the same.) They also function as a way for abortion foes to surround abortion with stigma and shame, and attempt to convince people that a common healthcare procedure is dangerous and immoral. D&E is a surgical abortion option in which a patient’s cervix is dilated and the fetus is removed via suction and with the help of additional surgical tools, like forceps, if necessary. It is a safe and trusted procedure with minimal complications, but it has been villainized by the right, who refer to the method as “partial-birth abortion,” a term that is deliberately inflammatory and, according to the Guttmacher Institute, “has no precise medical definition.”
“Texas has been hellbent on legislating abortion out of existence, and it is galling that a federal court would uphold a law that so clearly defies decades of Supreme Court precedent,” said Nancy Northup, president and CEO of the Center for Reproductive Rights. “At a time when the health care needs of Texans are greater than ever, the state should be making abortion more accessible, not less.”
Other states—Arizona, Georgia, Kentucky, Michigan, and Mississippi—have already adopted a slew of similar laws based on medically unfounded anti-abortion hogwash. This move by the Fifth Circuit only emboldens them, and any other states that wish to follow suit. And with a majority conservative Supreme Court, the future of abortion rights in the United States has only become increasingly bleak.
But abortion funds are never unprepared for battles like this one. Organizations like Lilith Fund and Texas Equal Access Fund, nonprofits that provide financial assistance and emotional support for those seeking abortions in Texas, are implementing donation drives with extreme urgency as they await a future that may require them to help people seek abortions out of state.https://jezebel.com/embed/inset/iframe?id=instagram-CSc-h19r4A9&autosize=1
This is work that continues no matter what the law says—even with Roe on the books, even without S.B. 8, access to abortion is still something advocates fight for every day.Subscribe to our newsletter!Don’t miss Jezebel’s top stories. Sign up for our daily email:Type your emailSign Me UpBy subscribing you agree to our Terms of Use and Privacy Policy.
“I want people who need abortions to know that they can depend on abortion providers, funds, advocates to not only fight for the right to a legal and safe abortion, but a world where abortion is accessible,” said Paige Alexandria, a board member and former client of Lilith Fund, in the organization’s latest video. “Regardless of your zip code or how much money you make.”
Measures would ban abortion if there is indication of fetal diagnosis in the patient’s reason and grant new “personhood” rights for fetuses and embryos.
The Center for Reproductive Rights and its partners have filed a lawsuit today challenging two Arizona abortion restrictions. One would ban abortion if there is any indication that the patient’s reason is a fetal diagnosis; the other would grant “personhood” rights to fetuses, embryos, and fertilized eggs in a manner that threatens to criminalize essential medical care for pregnant patients and other actions by pregnant people.
The lawsuit, filed in federal district court in Arizona, aims to secure a preliminary injunction before the measures take effect on September 29, 2021. The plaintiffs in the suit—two Arizona physicians, the Arizona Medical Association, National Council of Jewish Women Arizona, and the Arizona National Organization of Women—are being represented by the Center, the American Civil Liberties Union, and the ACLU of Arizona.
“Politicians should not get to decide what an acceptable reason is for seeking an abortion,” said Emily Nestler, Senior Counsel at the Center. “This law is an affront to our constitutional rights and our ability to make private decisions free from government intrusion.”
The law being challenged, S.B. 1457, adds a fetal diagnosis reason ban to Arizona’s existing sex and race reason bans enacted in 2011. The ban would target pregnant people already facing complex decisions regarding fetal genetic conditions, taking away their constitutional right to choose a pre-viability abortion. The law’s “personhood requirement” would anoint fetuses, embryos, and fertilized eggs with the same “rights and privileges” as “other persons” starting at the point of conception for purposes of all Arizona law. This sweeping change threatens both health care providers and pregnant women with criminal liability for a wide range of actions that could impact a pregnancy.
Numerous Restrictions Make Abortion Care Difficult to Access in Arizona
Arizona has several existing abortion restrictions that make it difficult for people to access abortion, including a mandatory 24-hour waiting period for people seeking abortion; a ban on the use of telemedicine for medication abortion services; and a law banning advanced practice clinicians like nurse practitioners from providing abortion care. If the U.S. Supreme Court overturns Roe v. Wade, Arizona and nearly half the states in the country are poised to ban abortion entirely. (See the Center’s “What if Roe fell?” abortion laws map here for more information on Arizona’s abortion restrictions.)
“These extreme restrictions are just the latest attempt by Arizona’s anti-abortion lawmakers to outlaw abortion care in their state,” said Nestler. “We will continue to fight for the people of Arizona and other states to ensure they can exercise their constitutional right to make decisions about their bodies and their futures.”
This fall, the U.S. Supreme Court will hear oral arguments in the Center’s case, Dobbs v. Jackson Women’s Health Organization.In the case, Mississippi has asked the Court to overturn Roe v. Wade and allow states to ban abortion before viability.
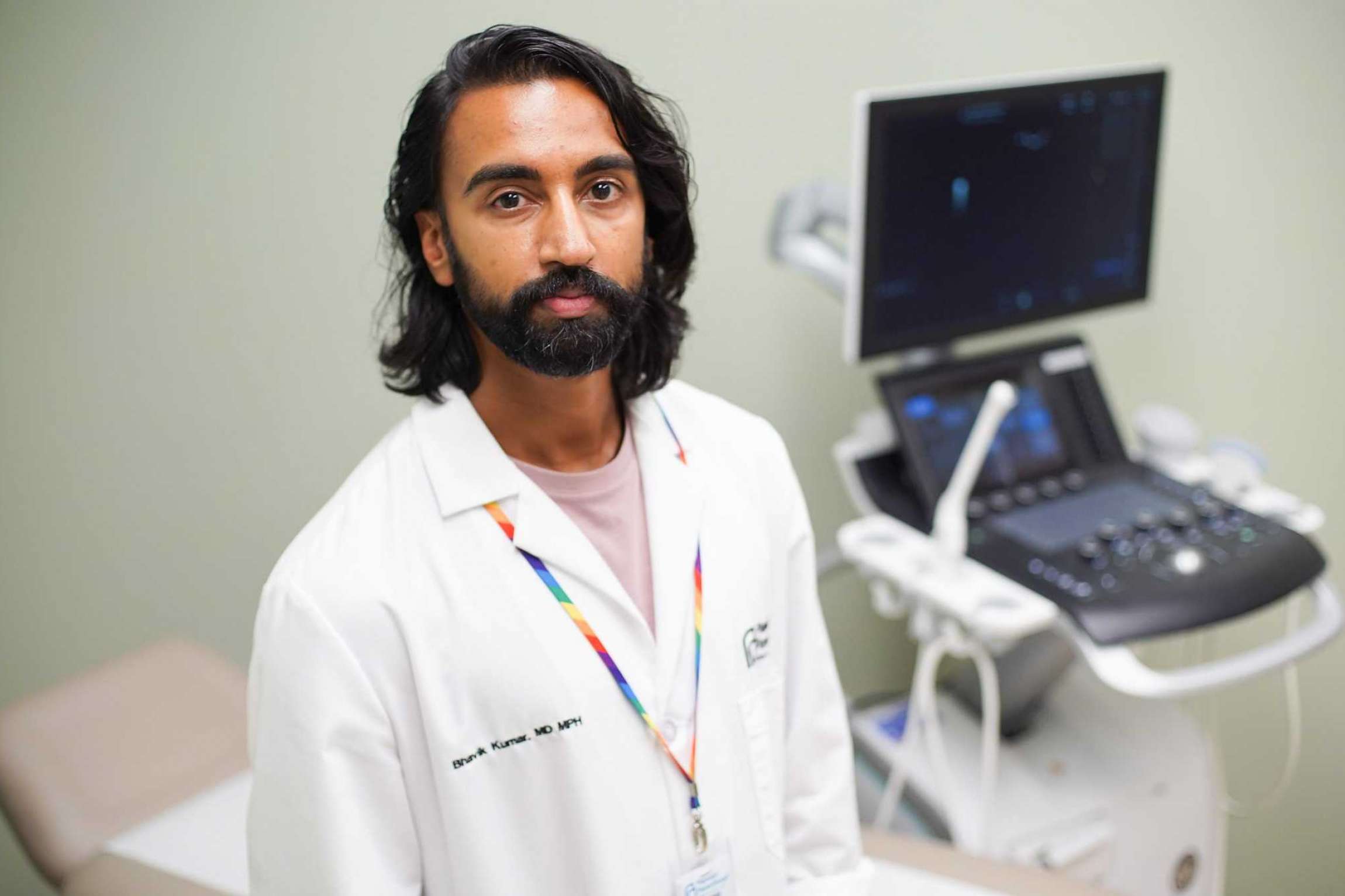
Dr. Bhavik Kumar, an abortion provider for Planned Parenthood, has cleared his schedule to fit in as many patients as he can before Texas’ restrictive abortion law goes into effect Sept. 1.Elizabeth Conley, Houston Chronicle / Staff photographer
The National Abortion Federation has told doctors in Texas it will stop referring patients and sending money to clinics that offer abortions after about six weeks of pregnancy.
In North Texas, the Texas Equal Action Fund will likely “pause” its ride-share program that helps women reach abortion appointments.
Dr. Bhavik Kumar, an abortion provider for Planned Parenthood, has cleared his schedule to fit in as many patients as he can before the end of the month.
And online, the group Texas Right to Life has launched a website for whistleblowers who want to potentially help sue Kumar and doctors just like him, beginning Sept. 1.
With only days left until the country’s first six-week abortion ban rolls out in Texas, abortion clinics and their supporters are bracing for a virtual shutdown of legal access to the procedure, at least for several weeks. Some clinics in the state are preparing not only to abide by the new guidelines but to go beyond them, shuttering their abortion offerings entirely.
“This law is senseless. It’s not in the best interest of the people of Texas,” Kumar said. “But it is the law, and if it passes, we have to comply.”
What unfolds over the coming weeks could have broad ripple effects. Even a brief pause in access in Texas, the second most populous state, could affect thousands of pregnant women and encourage similar laws across much of the South and Midwest, where abortion care is already limited.
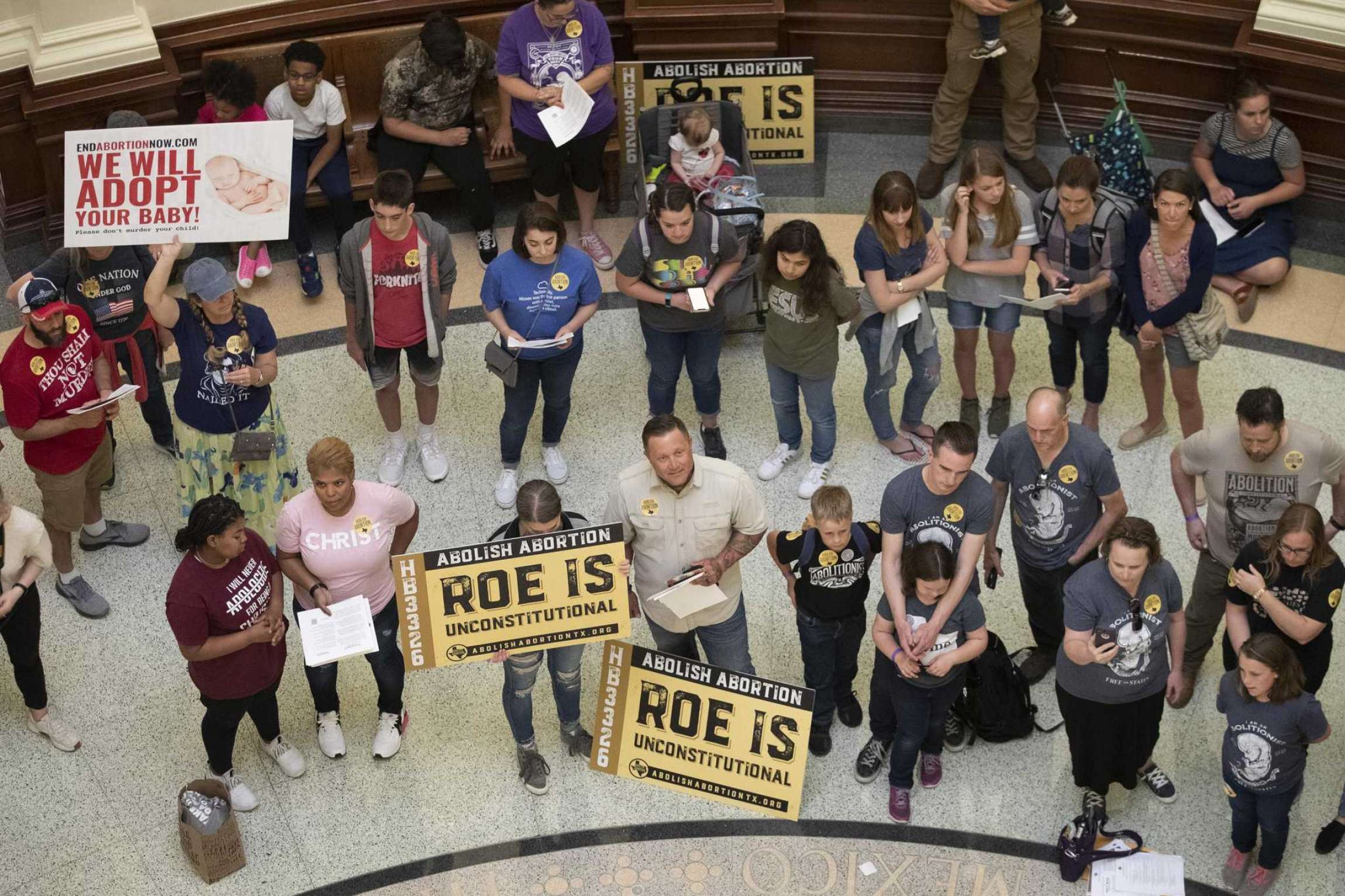
In this March 30, 2021 file photo, anti-abortion rights demonstrators gather in the rotunda at the Capitol while the Senate debated anti-abortion bills in Austin, Texas. Abortion-rights groups are challenging a new Texas law that bans abortions after six weeks of pregnancy and allows private citizens to file their own lawsuits as a way to enforce the ban. Texas is among several states passing abortion restrictions as the U.S. Supreme Court prepares to hear a case that could undo decades of abortion rights. (Jay Janner/Austin American-Statesman via AP, File)Jay Janner, MBR / Associated Press
“This is a new approach, and it’s going to open up new opportunities,” said John Seago, legislative director for Texas Right to Life, which opposes abortion access. “It’s a different battlefield than what we typically have with pro-life laws, and that’s why we’re optimistic.”
Abortion providers are trying to delay the rollout in federal court but are not counting on a win given the law’s largely untested enforcement tool. Unlike similar bans in other states, which have all been blocked by judges, Senate Bill 8 allows ordinary citizens to sue doctors and others who defy the ban.
That makes it tough to challenge preemptively, because providers don’t know whom to sue.
Hundreds of Texas lawyers have come out against the law, warning it contradicts provisions in the state constitution and would open the door to absurd outcomes beyond abortion if allowed to stand. Even proponents of the law expect many of the suits to be dismissed.
But providers and the people who help women access abortions in Texas say they can’t afford the risk of potentially endless litigation, even if hardly any of it is deemed credible. Under the law, defendants are unable to recoup legal expenses.
That’s why some are considering shutting down their abortion operations altogether, at least until it is clear whether the law will withstand scrutiny in the courts.
“I have one physician who’s for sure willing to provide abortions and comply with SB 8,” said Amy Hagstrom Miller, the chief executive of Whole Woman’s Health. “But the rest of my 16 physicians are still trying to figure out where their risks stop and start, and if they’re willing to provide.”
Defying new law not a popular option
Most of the physicians at Whole Woman’s four clinics in Texas also work at universities and in other states, flying in regularly to provide abortions. Hagstrom Miller said she does not plan to shut down any of the sites, regardless of the law, and will continue at least providing nonabortion pregnancy care, as well as counseling and referrals to clinics in states where abortion access is more protected.
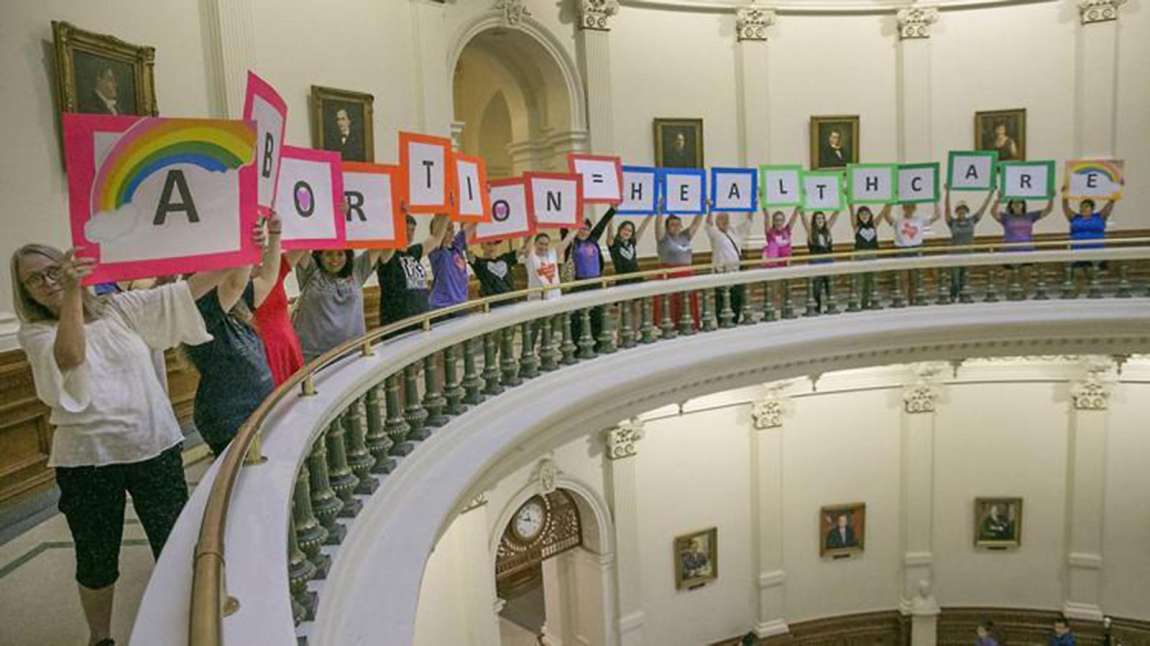
Abortion rights advocates protest abortion restrictions being debated in the Texas House on July 2017 at the Capitol. (RALPH BARRERA/AUSTIN AMERICAN-STATESMAN/TNS)RALPH BARRERA, MBR / TNS
Dr. Lauren Thaxton, a Whole Woman’s provider and a researcher at the Texas Policy Evaluation Project who is still weighing her options, said she assumes she will be sued even if she tries to provide abortion care strictly within the parameters of the law.
“Whether or not a case is found to be reasonable, or a true violation of SB 8, there are concerns about how that could affect someone’s other sources of employment,” she said. “How that could affect their medical licensing. How that could affect the patients that they see and their potential loss of privacy.”
Thaxton and others said they were unaware of anyone who is planning to openly defy the law on Sept. 1, though that strategy has been discussed.
Planned Parenthood Gulf Coast, where Kumar works, will continue offering abortions for women before the fetal heartbeat has been detected, as allowed under the law. But most women don’t know they’re pregnant at that point, typically about six weeks into the gestation period.
Spokeswomen at the nonprofit’s two other independent Texas affiliates, one based in San Antonio and the other in Dallas, declined to describe their plans.
Kumar said “the vast majority” of Planned Parenthood patients will need to leave the state for abortion care if the law proceeds, and that he is personally preparing to pitch in at out-of-state clinics that accept Texas patients, to help with their influxes.
Providers performed about 54,000 abortions last year and 56,000 in 2019, according to state data.
The chaos now forming may be the exact scenario that lawmakers were envisioning when they passed Senate Bill 8 this spring. Republicans, who control all branches of the Texas government, have tried for years to choke the industry out of existence, imposing restriction after restriction, many of them later overturned in federal court.
Past disruptions, including last year when Gov. Greg Abbott prohibited most abortions at the beginning of the COVID-19 pandemic, have especially impacted low-income women and women of color, many of whom lack private insurance or the resources or time to travel out of state, according to groups that support abortion access.
‘They think they can go to jail’
This upheaval could drag on longer, and it’s not clear that providers would be able to outright block the law even if they prove that it infringed on their federally protected right to abortion. Josh Blackman, a constitutional law professor at South Texas College of Law Houston, said the decisions in each suit will apply only to that case.
“This is a law designed to prevent Planned Parenthood from going on offense,” he said. “It keeps them on defense.”
In response, abortion providers and their support networks in Texas are scrambling to expand the out-of-state pipelines they pieced together last year and that many have feared will be needed if the conservative-led U.S. Supreme Court rolls back federal abortion protections. This fall, the justices are set to hear their first major abortion case in years.
At abortion clinics, employees are being retrained on what information they will be able to legally give patients on Sept. 1. Those who choose to comply with the law will have to update their websites and promotional materials.
Earlier this month, the National Abortion Federation, a coalition of abortion providers, notified clinics in Texas that it would be pulling support from clinics that defy the ban but would fund up to the full cost of patients seeking abortions within the new guidelines. Chief executive Katherine Hancock Ragsdale said in an interview that the organization is creating a special “concierge team” to assist women in Texas.
Small abortion funds that operate solely in Texas are also rethinking their approach and have been inundated with questions internally.
“No one knows what’s happening. Even our volunteers, they think they can go to jail when that’s not what this is,” said Kamyon Conner, who heads the Texas Equal Access Fund.
Despite the rhetoric, abortion opponents and others are not convinced that providers will comply with the law. Many of their supporters have been working for months to recruit women and employees at abortion clinics who would be willing to help sue. Successful claimants can win at least $10,000 in damages.
“There’s a lot of people who are interested in this fight from different angles,” said Seago, of Texas Right to Life. “And you’re going to see a lot of these people getting involved, now that they have the tools to do it.”
The Reproductive Freedom Act is intended to go beyond the status quo of Roe v. Wade, Sheila Reynertson of the New Jersey Policy Perspective said. “Roe hasn’t protected all communities.” Shutterstock/Rewire News Group illustration
But the Reproductive Freedom Act remains stalled despite support from New Jersey Gov. Phil Murphy and most New Jerseyans.
Every day that New Jersey’s Reproductive Freedom Act remains stalled in legislative committee is another day that patients in the state are scrambling to put funds together and make travel plans to access abortion.
That’s the scene set by Sheila Reynertson, senior policy analyst with the nonpartisan think tank New Jersey Policy Perspective.
New Jersey Policy Perspective is part of Thrive New Jersey, a coalition of 44 advocacy groups, health-care providers, and religious leaders organizing to pass the Reproductive Freedom Act. Introduced in October, the RFA would “explicitly guarantee, to every individual, the fundamental right to reproductive autonomy, which includes the right to contraception, the right to abortion, and the right to carry a pregnancy to term.” It would also ensure that no legislation or regulation could be passed to limit that right to New Jerseyans.
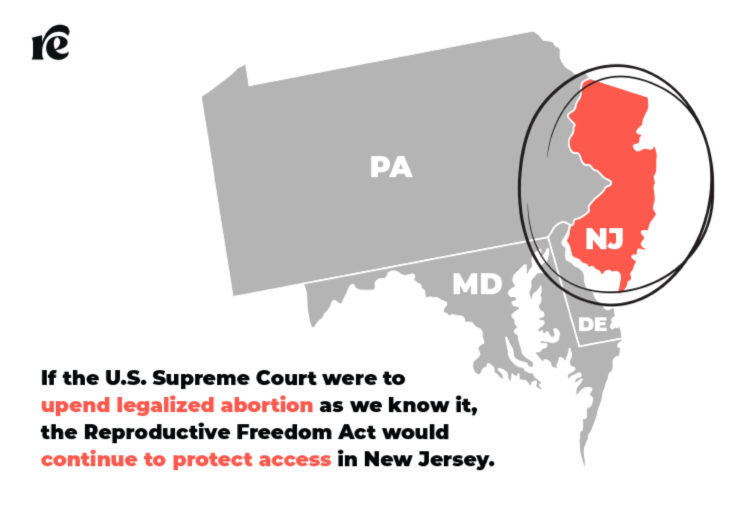
That means if the U.S. Supreme Court were to upend legalized abortion as we know it in Dobbs v. Jackson Women’s Health Organization, the Reproductive Freedom Act would continue to protect access in New Jersey. (The Supreme Court will hear arguments in the case in the fall, with a ruling expected around next June.)
“This is needed; this is urgent; this is not a matter where we want to wait for the Supreme Court to act,” said Anjali Mehrotra, president of NOW-NJ, a member organization of Thrive New Jersey. “We don’t want to be reactive—we want to be proactive.”
The RFA would:
require insurance plans in New Jersey to cover abortion and at least 12 months of contraception
allow a wider range of medical practitioners to provide abortion
modernize outdated language in state laws that could be used to criminalize pregnancy loss
update the language of state laws to be inclusive of trans and nonbinary people
The legislation is intended to go beyond the status quo of Roe v. Wade, Reynertson said.
“From day one, we didn’t want this to be a ‘codify’ bill—we wanted it to expand people’s rights,” she said. “We were very frank that no, actually, Roe hasn’t protected all communities.”
A logistical hassle
You might not think of New Jersey as a state where folks would need to travel hours to access abortion, but that’s the reality for many patients, according to Roxanne Sutocky, patient coordinator at the Cherry Hill Women’s Center.
The RFA would enable health-care professionals like nurse practitioners and midwives to provide abortion, which providers say would be a game-changer for patients in underserved parts of the state. About a third of New Jersey counties lack an abortion provider, and for some people, traveling out of state might be the closer option.
“People in the southern part of the state may have to travel to Delaware and Pennsylvania for the nearest abortion providers,” said Casey Olesko of Planned Parenthood of Northern, Central, and Southern New Jersey.
The RFA would also reduce barriers to later abortion by cutting through regulatory red tape that prevents qualified abortion providers from offering later abortions. New Jerseyans must fly to other states to access abortion later in pregnancy because it is not available in the state, Jada Grisson of the New Jersey Abortion Access Fund said.
But those logistics don’t come together easily, particularly for a working parent. And considering that around 59 percent of abortion patients are already parents, patients often need to take time off work, find child care, and come up with the money needed for both the travel and the procedure itself, leaving access out of reach for many.
Thrive New Jersey members also want to provide a safe haven of abortion access for people traveling from more restrictive states. The New Jersey Abortion Access Fund reported a spike in requests for funding from other states, which they attribute to the pandemic and new abortion restrictions, particularly during a year as volatile as 2021 for abortion rights. States passing a record-number of abortion restrictions has ripple effects across the country.
“Things in Texas affect people in New Jersey, and things in New Jersey affect people in Texas. Our freedom is a national issue,” said Rabbi Philip Bazeley, one of 55 faith leaders to sign an open letter in support of the RFA. “We also see it as a racial justice issue—many of these laws are going to affect minority ethnicities at a greater rate than others.”
Thrive coalition members say the RFA was drafted with the intent of centering the concerns of marginalized communities. In New Jersey, state funding for undocumented people’s health care covers birth control and prenatal care but not abortion. The RFA would change that. The legislation also uses gender-neutral language to describe pregnancy, and has received endorsements from LGBTQ rights groups Garden State Equality and HiTOPS.
The coalition has faced challenges as various organizations came together under one umbrella. Mehrotra, the president of NOW-NJ, said Thrive New Jersey has had to address concerns about its mostly white leadership.
“I felt that I had a seat at the table, but not in the decision-making,” Mehrotra, who is South Asian, said. “I spoke up, and it was not the easiest thing to do, but I’m really glad I did because it was taken really well. We ended up really changing the entire structure of the coalition—the response was tremendous.”
Mehrotra said studying coalition work in other states, with the help of national partners, helped Thrive grow into a more inclusive coalition.
“We are at a stalemate here,” Reynertson said. “The legislative leadership also thinks there’s no [access] emergency in New Jersey.” She added that the Democratic-controlled legislature needs to create more pressure to advance the legislation.
Mehrotra remains optimistic that the bill will pass after New Jersey’s off-year elections in November, but she’s hoping lawmakers act before the Supreme Court rules on Jackson Women’s Health.
“I think people outside of the state make a lot of assumptions—they look at blue states and think, ‘At least you don’t have heartbeat bills,’” Grisson said. “My biggest hope is to see that financial barrier removed because abortion has been legal only in theory for too long.”
![Demonstrators in favour of legalising abortion react after the Senate passed an abortion bill, in Buenos Aires, Argentina on December 30, 2020 [File: Reuters/Agustin Marcarian]](https://www.aljazeera.com/wp-content/uploads/2021/08/2020-12-30T104927Z_439396987_RC2MXK96R5K9_RTRMADP_3_ARGENTINA-ABORTION.jpg?resize=770%2C513)