Demand for telemedicine drastically increased during the COVID-19 pandemic, but conservative lawmakers have effectively banned remote access to abortion care in at least 19 states. Shutterstock
Abortion is incredibly safe, and so is telemedicine abortion. A federal judge in Indiana agreed.
A federal judge permanently struck down Indiana’s ban on telemedicine abortions last Tuesday, along with a host of other abortion restrictions in the state.
Indiana law prohibits telemedicine abortion and requires patients to be examined in person to receive abortion care. While Indiana officials claimed these laws are necessary for safety, Judge Sarah Evans Barker of the Southern District of Indiana ruled that the state was unable to prove telemedicine abortion is unsafe.
“The State’s attempt to explain its basis for excluding the far-reaching benefits of telemedicine from [abortion] patients is feeble at best, especially given the widespread use of telemedicine throughout Indiana as well as the overall safety of medication abortions,” Barker wrote in a 158-page ruling.
Barker is entirely correct. Abortion is incredibly safe, and so is telemedicine abortion. (For more on this, check out our collection of reporting on medication abortion as the future of abortion access.) There is no good reason for lawmakers to restrict access to it, except as part of a ploy to decimate abortion access overall.
The ruling came in response to a 2018 lawsuit challenging dozens of Indiana abortion restrictions, filed on behalf of Whole Woman’s Health Alliance and All-Options Pregnancy Resource Center.
a law preventing qualified nurse practitioners from providing medication abortions
a requirement that second trimester abortions be provided in hospitals or ambulatory surgical centers
a forced counseling law that makes abortion patients sit through misleading information on “fetal pain” and other false claims
and several TRAP laws (targeted regulation of abortion providers).
At the same time, however, the court upheld a number of other abortion restrictions challenged in the lawsuit.
But the court’s decision to strike down the telemedicine ban comes at a critical time. While demand for telemedicine drastically increased during the COVID-19 pandemic, conservative lawmakers have effectively banned remote access to abortion care in at least 18 states besides Indiana.
And the fight isn’t over in Indiana: Only a day after the ruling, Indiana Attorney General Todd Rokita appealed the decision to the Seventh Circuit Court of Appeals.
In August of 2017, ReproAction and SisterSong joined forces to protest fake abortion clinics in Atlanta (ReproAction)
Organizations like SPARK, ReproAction and Abortion Access Front are exposing the deceptive tactics of fake abortion clinics and organizing to stop them from harming women.
“My high school was down the street from a crisis pregnancy center. My house that I grew up in was next door to a crisis center. I drove by it every day and saw ‘pregnancy resource center.’ I just assumed that it was a medical provider. I wasn’t the only person fooled,” says Agbo Ikor, Director of Programs at SPARK Reproductive Justice NOW in Atlanta, Georgia.
“My best friend when she was pregnant, she was taken to a crisis pregnancy center. And while she was there, they shamed her. They made her feel like if she had an abortion she was just this terrible person. It was very traumatizing for her,” says Ikor. “It is infuriating. It’s just really, really hard to think about.”
Ikor and other activists across the country are fighting back against “crisis pregnancy centers” (CPCs)—called fake abortion clinics or anti-abortion centers by reproductive justice activists. SPARK, ReproAction and Abortion Access Front are leading campaigns to expose the deceptive and harmful tactics of anti-abortion centers and mobilizing activists to fight them.
What Are Anti-Abortion Centers and How Are They Funded?
While states have passed ever more restrictive abortion laws and closed down reproductive health clinics in increasing numbers over the last several years, anti-abortion centers have proliferated. There are currently about 2,700 anti-abortion centers across the United States, more than three times the number of reproductive health care clinics that provide abortion services.
Staff at anti-abortion centers wear surgical scrubs or white coats, they ask clients to fill out medical history questionnaires, they offer pregnancy tests and ultrasound scans, all in order to appear as if the center is a licensed medical facility—despite the fact that most are unlicensed and have no medically trained personnel on site. Many anti-abortion centers locate next to or across the street from full-service reproductive health centers and use similar-sounding names.
Activists note that these tactics sometimes make it hard to tell the difference between a real clinic and a fake one. “They’ve gotten wise to this larger movement calling them out and they started adapting,” said Anna Bean, Director of Programs of the Abortion Access Front. “So they’re constantly changing their names, adopting more feminist terminology on their websites. They use the language of choice and empowerment and knowledge and all the things that we want reproductive healthcare to be about. They’re manipulating that, like a fake clinic used to be called ‘St. Joseph’s Crisis Pregnancy Center.’ Now, it’s like, ‘Options for Women.’ It’s harder to figure out if it’s a real clinic. They’re getting more hip to what’s going on.”
One of various posters and infographics created by ReproAction to demonstrate the harm of fake abortion clinics (ReproAction)
Fake clinics target the most vulnerable women, says Dr. Andrea Swartzendruber, who is a professor of epidemiology and biostatistics at the University of Georgia and researches anti-abortion centers.
“CPCs particularly target their advertising and services to some of the same groups who are most impacted by unintended pregnancy or sexually transmitted infections. And those include young people, especially young people who may be on their parents insurance and are looking for free services…and may be vulnerable to believing the misinformation that CPCs put out,” says Swartzendruber.
“In many places in Georgia and elsewhere, folks of color and people who live in low-income households are also really vulnerable to the attraction of CPC services, which are provided for free…CPCs try to target themselves to those populations.”
“The purpose of CPCs is to prevent people from making informed choices around their bodies and their pregnancies,” says Ikor. “One of the most maddening things about them is that they purport to offer low cost services, which a lot of Black people need, and then they actually are not accurate. That’s just really, really harmful, and really taking advantage of the fact that these resources aren’t available or accessible to low income folks or folks of color. That’s how they fit into the whole medical industrial complex and medical racism as a whole.”
While CPCs appear to be local, community-based organizations, they are usually part of large extremely-wealthy networks, such as Heartbeat International, Birthright International, Care Network, National Institute of Family and Life Advocates, or Human Coalition, says Shireen Shakouri, Deputy Director at ReproAction. “They seem more community oriented than they actually are, but they are widely-tentacled organizations and very technologically savvy,” says Shakouri.
“They have intense, highly-strategized marketing schemes to pull people in from the internet, whether it’s SEO manipulation or geolocation services. They are using every tool in their tool belt to find what they would call ‘abortion minded’ or ‘abortion vulnerable’ people and pull them into their clinics. And from there, the manipulation just accelerates.”
Image accompanying ReproAction blog by Shireen Shakouri on ‘Why Anti-Abortion Fake Clinics Aren’t Helping New Parents’ (ReproAction)
What’s more, anti-abortion centers receive a significant amount of state and federal funding. In a report released last June, Equity Forward revealed that state lawmakers are funding anti-abortion centers and diverting federal dollars earmarked for impoverished mothers and children to these centers.
During the Trump administration, the federal government granted $1.7 million in Title X funding—meant for family planning services—to the coercive Obria Medical Clinics, a Christian, antiabortion organization that opposes hormonal birth control and other contraceptives and offers training in the unreliable rhythm method.
For years, anti-abortion center networks have received federal sex education funds to run centers and teach abstinence-based education in public schools. But these groups are now applying for a wide range of federal grants, including ones earmarked for maternity group homes, youth homelessness, human trafficking, domestic violence prevention, teen pregnancy prevention, adoption and other child welfare issues.
In response, advocates across the country are organizing to prevent these centers from causing any more damage.
“We’ve created a lot of materials, encouraging people to protest fake clinics, to find ways to call them out, go to their fundraisers and go to events that they sponsor,” says Shakouri.
The fake clinic database lists anti-abortion centers by state, address, affiliation and whether they promote “abortion pill reversal”—“an unproven, unethical experiment performed on abortion patients, often without knowledge they are being experimented upon,” says ReproAction.
The direct action toolkit offers a step-by-step guide on how to locate fake clinics, how to plan a protest, best practices for non-violent direct action and how to write a letter to the editor. Before the pandemic, Shakouri held in-person trainings on how to counter fake clinics. She hopes to do so again soon.
“We’ve hosted a bunch of protests outside of fake clinics,” says Shakouri. “We want them to know we are watching them, we know who they are, and to let them know that we’re not going to let up until people actually know what they’re doing there.”
One of various images and infographics created by ReproAction to fight fake abortion clinics (ReproAction)
ReproAction is also working with local groups to protest anti-abortion centers conducting sex education in public schools, says Shakouri. “Municipalities don’t have their own budgeting for sex education so they are very happy to work with these organizations that are happy to do stuff for free because they have all this federal money. So you are getting very clearly ideologically-based, usually Christian-based, fake clinic organizations going into public schools and teaching their faith-based programming.”
In their in-depth investigations into the finances of these centers, detailed in the report The Big Money Behind the Big “Pro-Life,” ReproAction tracked the revenues and expenses of the largest anti-abortion organizations in the country. In 2016 alone, the top 15 organizations in the ‘pro-life’ movement had $197,457,166 total contributions and grants, $208,584,844 in revenues, $211,880,115 total expenses, and $3,769,128 in salaries to top-paid employees.
After learning that some of the big anti-abortion groups are providing guidance to anti-abortion centers on how to apply for federal grants, ReproAction organized a petition drive targeting Xavier Becerra, Secretary of the U.S. Department of Health and Human Services, demanding the agency give no federal funding to anti-abortion fake clinics. The petition states, “Funneling money to anti-abortion fake clinics was common in the previous administration. There is no excuse for continuing this practice now.”
ReproAction is also working with local activists on campaigns against state funding for fake clinics in North Carolina and Missouri.
Another key player in the fight against fake clinics is the Abortion Access Front (formerly Lady Parts Justice League), who describe themselves as “a coven of hilarious badass feminists who use humor and pop culture to expose the haters fighting against reproductive rights.” One of their major campaigns is to raise awareness about fake clinics.
“Direct action is our jam,” says Anna Bean, Director of Programs of the Abortion Access Front.
A week long protest held in Texas to ask for Gov. Greg Abbott (R-Texas) to defund crisis pregnancy centers (@urgergv / Expose Fake Clinics)
Abortion Access Front has organized several petitions to defund fake clinics, including one in 2019 against the Trump administration giving Title X funds to the Obria Group and another to protest CPCs receiving PPP loans.
Social media graphic to share Expose Fake Clinic’s petition to make fake clinics return their PPP loans (Expose Fake Clinics)
“Humor and satire are a really potent force for educating people and then making them angry,” says Bean. Abortion Access Front’s founder Lizz Winstead was the co-creator and head writer of Comedy Central’s The Daily Show.
“Everyone loves comedy and everyone deserves to have joy and laughter in their day. We want to make sure there’s a real space for laughter and joy and dancing. Not everything’s always funny all the time, but we found that that angle is a good hook, and it brings in more people that aren’t necessarily already in the fight. It gives people a more accessible sense that I can be part of this too.”
Activists with Abortion Access Front protesting fake abortion clinics (Abortion Access Front)
State Campaigns Against Fake Clinics
ReproAction and Abortion Access Front are supporting several state-based groups across the country on campaigns to fight anti-abortion centers in their states.
In 2017, activists in Hartford, Connecticut worked to pass a city ordinance to make anti-abortion centers’ deceptive practices more transparent. The ordinance requires fake women’s health centers to post a sign stating whether or not there is a licensed medical provider on the premises and available to provide medical services. It also prohibits fake women’s health centers from disseminating false, misleading, or deceptive information about the services they provide and from deceiving women into thinking that they provide specific services, like abortion, when they don’t. A legal challenge to the ordinance failed, and after the Supreme Court’s 2018 decision striking down a California law regulating fake clinics, the Hartford ordinance was modified but is still in effect.
Then in February of 2018, NARAL Pro-Choice Connecticut Foundation issued a research report documenting the deceptive practices of CPCs and pushing for a state law regulating them. And earlier this year, the Connecticut legislature passed a law that recently went into effect that prohibits fake clinics from engaging in false advertising.
Under the bill, the state attorney general may investigate complaints, and can fine centers up to $500 and charge “reasonable attorney’s fees and costs” if a court finds they engaged in deceptive advertising.
“Put simply, if you sell Subarus, don’t claim it’s a Mercedes-Benz,’’ said Connecticut Representative Christine Palm (D-Chester). “If you’re a bakery, don’t pretend that you sell fruit just because it’s another food item. If you’re a dentist, you’re not an epidemiologist, even though you’re in the medical field. And if you provide adoption counseling and you discourage people from getting abortions, don’t imply, suggest or insinuate that you do otherwise.’’
Other states have active campaigns as well. In Georgia, SPARK has joined together with several other organizations in the state—including Amplify Georgia, New Georgia Project, URGE, and Access Reproductive Care-Southeast—to fight fake clinics. The organizations formed a working group that runs a campaign called Fake Clinics Suck, working to educate the public about how fake clinics try to mislead people. They have a map of fake clinics on their website and hold town halls where people can share stories about their experiences with fake clinics.
“We want to educate the public around what they actually are, how they actually operate and why they’re harmful,” says Ikor.
The working group is also organizing to rescind state funds for fake clinics. In 2016, Georgia passed a law allocating $2 million to fake clinics. Ikor and others are working with Representative Renitta Shannon on legislation to defund them, and redirect the funding to other organizations that can provide comprehensive, unbiased medical care and pregnancy resources to low-income people.
“No One Should Be Lied To”
Advocates fighting fake clinics express their exasperation and rage about the harms of fake clinics.
“We’ve talked to a lot of abortion providers who have dealt with people who have gone to fake clinics. It’s just absolutely doubling down on the internal shame they already feel for seeking abortion and stigmatizing reproductive health care generally,” says Shakouri.
“People feel dumb. People feel even more afraid because they are told they could maybe die from their abortion, and that they’re just making the most selfish and awful decision. And they just feel even more confused and alone. One of the worst aspects of these institutions is they claim they love women, and they just want to save women and babies from this awful, awful thing, but instead they are absolutely exponentially multiplying the harm.”
Bean agrees. “There are so many things that are just so enraging about these fake clinics, but it’s still kind of flying under the radar. There’s so much they’ve been able to get away with saying it’s free speech. But you have a lot of power to educate folks about who’s operating or community and what deceptive practices they are using. I hope that people feel empowered to call their elected officials. You can also have a lot of fun standing outside with some fun signs, exposing them that way. So there’s a whole sort of range of ways that we can all be keeping that conversation alive and loud.”
“No one should be lied to,” Bean explains. “Everyone should have access to information and be treated with dignity and respect their health care decisions.”
We Testify abortion storytellers rally at Supreme Court for June Medical Services v. Russo oral arguments, March 2020. (We Testify)
What kind of nation allows people to be prosecuted for health care?
WASHINGTON, D.C.—Last November, I drove more than 12 hours for an abortion. It wasn’t mine (I had mine in 2005); I picked up a young woman in rural Pennsylvania whom I’ll call Raquel. She needed a ride to a clinic in Maryland to get some pills that she would take back at her home to have a medication abortion. As we drove to the clinic, I told Raquel about what to expect during the appointment; after I finished I paused and said, “As much as I love getting to know you on this drive, did you know you could safely do this at home but the government won’t let you?” She was surprised. Like many people, she knew about limitations on abortion but didn’t know that very safe and basic methods are being restricted because of outdated FDA regulations on how they can be dispensed. The drive bonded us—we still keep in touch, and she approved the inclusion of her story here—but it was an unnecessary exercise, one that antiabortion politicians created to make yet another constitutional right as inaccessible as possible. The cruelty of the barricades along the journey is the point.
Since Covid-19 hit, I’ve thought a lot about that drive with Raquel, particularly as people have reached out needing abortions. States have limited travel, issued stay-at-home orders, and required people to quarantine for at least two weeks. While several states declared abortion an essential service, others exploited the pandemic to shutter clinics. The future we have worried about was upon us in an instant. Patients had appointments canceled. Those who could afford it, or who knew about abortion funds, were able to travel to other states for care. The moment was both unprecedented and familiar. The uselessness of our nation’s health care system was showing, and became even more burdensome on abortion patients.
In a just society, Raquel (and anyone wanting an abortion but anxious about contracting Covid-19) could have ordered the necessary pills via telemedicine, online, or at a pharmacy, and completed the abortion at home. That’s the way many people around the world do abortion, because it’s incredibly safe and simple. That’s how Americans once did it. Concoctions were advertised in newspapers and shipped through the mail, or herbs such as pennyroyal and black cohosh root were made into teas. But since the late 1800s, abortion has been deeply criminalized, and if Raquel had ordered the pills online, she and the person who sent them would have risked prosecution and jail. Recently, Polish abortion activists reminded me that all of our laws governing abortion actually promote criminalization. (To be sure, those are different from medical practice regulations that ensure procedures are performed correctly.) Rules dictate how, when, where, and why someone can have an abortion, and mandate a series of physical and legal barriers one must cross. Wait too long because you can’t afford the procedure? You can be criminalized. Take pills at home with a parent because you couldn’t afford a procedure? You both can be criminalized. Have a miscarriage, but a doctor thinks you self-managed an abortion? You can be criminalized. It doesn’t matter whether the rules are medically necessary or just, and of course, enforcement and punishment are significantly more severe with overpoliced communities of color and those who live in poverty.
What kind of nation allows people to be prosecuted for health care?
On July 13, just as this article was nearing publication, a federal judge issued an injunction on in-person requirements for dispensing pills necessary for a medication abortion, saying they create a “substantial obstacle” for patients, and may be an unconstitutional undue burden during a pandemic. The ruling allows providers to mail or deliver the pills to patients—an important step, however temporary, in jurisprudence and in people’s lives.
But this moment has radicalized me. I’ve never supported restrictions—I’ve experienced the panic they create when I was unsure if I could afford an abortion—but I’ve realized that it’s time for us to push for decriminalization of abortion and the abolition of all abortion restrictions. There is no medical necessity for any of these laws restricting abortion. They just create a tightrope for people to fall from and then invite the police into the experience.
As Black Lives Matter protests have swept our country, we are having a national dialogue about the spaces and places police hang around to control Black and brown people—schools, hospitals, grocery stores, coffee shops, and our homes. Police are heavily involved in our inability to exercise reproductive freedom; they brutalize us while pregnant; spray us with tear gas, which can affect our fertility;arrest people who choose to terminate a pregnancy outside of the narrow confines of the law; shoot our children; and shackle us during labor. We deserve police-free pregnancies. This is why the fight for reproductive justice is critical. It addresses systemic issues that have long prevented families of color from thriving on our own terms. It’s worth recalling that antiabortion white supremacists pivoted from rallying for school segregation to protesting abortion; they want to control our futures.
If we are serious about protecting abortion access, we have to become serious about the fight to abolish abortion laws. Our ancestors worked hard to ensure we had access to abortion to space our pregnancies, save our lives, and free us from the rape and violence of chattel slavery. It is in their tradition that we must continue to make abortion free and available, whenever and wherever someone needs it.
Covid-19 brought a taste of what life would be like if abortion were illegal again, but it always has been in some form through the criminalization of Black and brown bodies. I hope that more people will realize that to have reproductive justice, we have to take extreme efforts to decriminalize our health care, defund the police, and create communities that love people who have abortions, unapologetically.
Photo illustration by Slate. Photos by Fred Schilling/United States Supreme Court, United States Supreme Court, and Franz Jantzen/United States Supreme Court.
Does that mean it might be safe?
One of the most interesting fissures that has opened up within the conservative legal movement in recent years has been between mainstream conservative lawyers and the growing performance artist faction of the lawyers for the Trump base. Soon, the conservative justices themselves will have to pick which side of the battle they are on: With the filing last week of a brief that explicitly asks the Supreme Court to overturn Roe v. Wade, the state of Mississippi is forcing the court’s three newest Trump-appointed justices to choose between institutional stability and law that channels right-wing internet memes.
Examples of the latter abound in the past year. Rudy Giuliani has seen his license to practice law temporarily suspended—twice!—as a result of his star turns as all-purpose lawyer for crazy stuff. Last December, 17 Republican attorneys general signed a brief supporting a suit filed by Texas Attorney General Ken Paxton seeking to set aside the 2020 election based on false claims of “unconstitutional irregularities.” The chief law enforcement officers of those 17 states actually asked the Supreme Court to throw out every vote in the four consequential states in which Joe Biden had prevailed—Georgia, Michigan, Pennsylvania, and Wisconsin—and then have each state’s legislature declare Donald Trump the winner. Another exhibit might be the various lawsuits filed by Trump’s “Kraken” lawyers Lin Wood and Sidney Powell, who currently face the prospect of legal sanctions for their work advancing his bogus claims of a stolen election.
These filings bear certain hallmarks of what can best be described as litigation as imagined by a.m. talk radio hosts: maximalist claims, shoddy command of legal doctrine, disregard for the role of precedent, reliance on internet claims as “facts,” and a heavy dose of “own the libs” trolling. Distressingly, more and more frequently, these filings also bear the signatures of state attorneys general using the courts to advance their own political careers, as opposed to a coherent theory of justice. As Mark Joseph Stern explained, in describing why a full one-third of the nation’s attorneys general opted to use the power of their offices to sign on to a meritless effort to thwart democracy last December, “these lawyers run large agencies that deal with complex legal disputes every day; the job requires a level of competency that could not be met by someone suffering a complete break with reality. We should assume that these attorneys general are rational actors, politicians looking out for their own best interest.” As a result, he concluded, we must understand their willingness to sign on to the brief as an act of performative fealty to the Trump voters in their states. That these AGs have independent legal obligations and ethical rules that bar them from knowingly signing on to frivolous pleadings matters less than advancing Trump’s and their own future electoral fortunes, in their overarching calculations.
The brief filed Thursday by Mississippi Attorney General Lynn Fitch in Dobbs v. Jackson Women’s Health Organization, the most consequential abortion case of the past three decades, shows at least some signs of being a sober piece of legal pleading. It contains case citations and makes no mention of unsourced conspiracy theories. Yet in many respects, it also has some telltale whiffs of the Kraken, not least among them the headline-producing fact that the state explicitly asked the high court to overturn both Roe v. Wade and Planned Parenthood v. Casey. This request, only the third time a main brief has asked the court to overturn Roe since the case was decided and the first time in three decades, was a big, politically motivated swing directed at a court that may not be inclined to take a big politically motivated swing at Roe this fall.
The issue in Dobbs is the constitutionality of Mississippi’s Gestational Age Act, passed in 2018, among a raft of unconstitutional new anti-abortion laws in several states. The act forbids abortions after 15 weeks of gestational age unless in the case of a medical emergency or severe fetal abnormality, and offers no exceptions for cases of rape or incest. The law was challenged successfully by the only clinic in the state, and a federal appeals court agreed that the law was clearly an unconstitutional ban. Having hemmed and hawed and dithered, the Supreme Court finally agreed to hear the case in May, and made plain that the justices were prepared to explore whether states should be allowed to ban abortion prior to fetal viability, which occurs around 24 weeks of pregnancy. Viability has long been the dividing line that the Supreme Court has used to determine when a state can ban abortion—before viability, states must allow abortion (although they can impose certain barriers); after viability, states can ban the procedure as long as there are exceptions for the patient’s life and health. Arguments will likely take place in November or December with a decision to come before July.
Fitch’s brief represents an astoundingly maximalist theory of ignoring precedent, claiming that “the stare decisis case for overruling Roe and Casey is overwhelming.” Calling Roe v. Wade “egregiously wrong” (five times!), the brief asks the court to simply overturn every abortion rights decision made over the course of half a century. The casual trolling is indeed epic. Justice Ruth Bader Ginsburg, who dedicated her life to protecting women’s reproductive rights, is invoked to support the proposition that Roe and Casey “have inflicted significant damage” upon the country. The brief blames Roe for creating a national culture war that was in fact produced almost singlehandedly by Pat Buchanan, Phyllis Schlafly, and Nixon strategist Kevin Phillips. It contends that Roe and Casey and their progeny are not really precedent because they were fractured opinions. It argues that “abortion jurisprudence has harmed the Nation.” The brief even cites one of us (Lithwick) to support its claim that abortion is so contentious that it must be returned to the states to decide, without interference from the federal government. Trolly.
Just over one year ago, the Supreme Court struck down a Louisiana law that would have reduced the number of clinics in the state to one, and five years ago, the court struck down a Texas law that would have cut the number of clinics in the state by three-quarters. In neither of those cases did the state attorneys general, both outspoken, politically motivated, anti-abortion conservatives, urge the court to use the lawsuit to overturn Roe. So what changed?
Several things. For one, the Mississippi law at issue in this case is one of a new breed of extreme anti-abortion laws that have swept the nation in the past two years. Despite the fact that fetal viability is currently set at between 23 and 24 weeks, states have been banning abortion at 15 weeks (Mississippi, in this case), 12 weeks (Arkansas), 8 weeks (Missouri), 6 weeks (Ohio, Georgia, and seven others), and at conception (Alabama, Louisiana, Utah). In other words, these new laws are rooted not in state solicitude for public health, but in a desire to end legal abortion. Dobbs is the first case to arrive at the Supreme Court addressing these direct attacks on Roe.
Beyond that, the most essential change here is that Trump struck Republican gold during his presidency and was able to appoint three new Justices to the court. All three—Neil Gorsuch, Brett Kavanaugh, and Amy Coney Barrett—were established conservative jurists at the time they were elevated to the court, but by being appointed by Trump, and sometimes with some discomfort, their reputations and careers became reoriented as Trump loyalists. Since Trump stated that one of his chief goals in his court appointments was to appoint justices who would overturn Roe, Fitch received the precise message a loyal Trump soldier was sent loud and clear—send these justices a Trump-inspired brief that will appeal to the Trump moment. And that she did. What she may have missed is how hard the three Trump justices have labored to show the country that they are not partisans, not shoddy hacks, and not the brazen political actors their party promised. Just as the last term showed that, in some areas, minimalism and moderation were to be the lodestars of, at minimum, Barrett and Kavanaugh, Fitch served up a giant partisan fireworks display that would benefit her own image and career more than the Trump justices’. But perhaps that was the intended purpose.
Her Trump-stylized arguments certainly garnered immense attention for Fitch last week. Whether it further inclined the Supreme Court to grant the relief she sought is a much harder question. So far on the court, the Trump three have been reliable conservative votes, but they have not completely walked the party line. Gorsuch wrote the pivotal decision in 2020 giving LGBTQ people equal rights in the workplace; Kavanaugh is now the court’s median justice and cited something akin to the public perception of critical race theory in his opinion supporting college athletes against the NCAA; and Barrett stopped short of overturning a precedent about religious liberty that has been in conservative crosshairs for decades. These three are conservatives, there’s no two ways about it. But, are they bomb-thrower justices, like Samuel Alito and Clarence Thomas? Or are they justices prone to taking less visible, headline-eluding smaller steps to accomplish larger conservative goals while still paying some respect to half a century of precedent? That’s the choice before them now that Mississippi has so clearly thrown down the gauntlet.
Abortion rights activists who seek to see Roe ended outright celebrated the in-your-face-ness of the AG’s filing. Several argued that there was no other avenue for Mississippi and applauded the candor of a brief that no longer covered itself in fabrications about the real goals of the anti-choice movement. But, there is at least some reason to doubt that there are five, let alone four, or even three votes, at the high court for an in-your-face reversal of Roe just weeks before the 2022 midterm elections. It will be up to the Trump justices to decide just how much they side with the church of Trump, instead of the institution of the Supreme Court.
Activists supporting legal access to abortions protest during a demonstration outside the Supreme Court on March 4, 2020.Saul Loeb / AFP via Getty Images file
“Over the past year, we’ve seen states really target medication abortion in a way that we hadn’t seen,” Elizabeth Nash, of the Guttmacher Institute, said.
WASHINGTON — The coronavirus had started to shut much of the country down in March 2020 when Larada Lee found out she was six weeks pregnant.
She wanted to end her pregnancy and decided that instead of a surgical abortion, she would use medication, a process she could complete at home. This, she thought, was her best chance of limiting her exposure to Covid-19.
But Lee, then an Ohio State University student, was still forced to make a series of in-person doctors’ visits before she could get access to the drugs — all while grappling with the frightening new pandemic reality. Even then, she was still required to pick up the two-pill regimen at a health clinic, taking the first, mifepristone, there and the second, misoprostol, at home 24 hours later.
“Accessing abortion feels like one of the worst games of Tetris,” she said. “I am working full time and in school and I have hopes and aspirations for myself that would not be attainable if I was a parent.”
Women facing stay-at-home orders in other states have had an easier time getting prescriptions — through telehealth appointments. In an effort to expand access, the Food and Drug Administration temporarily eased long-standing in-person dispensing requirements for mifepristone — first in July 2020 in response to a court order that was later reversed by the Supreme Court, and again in April — so that women could order the pills by mail for the duration of the pandemic.
The agency’s move, along with the explosive growth in telehealth services and increase in self-managed medication abortions, sparked a flurry of legislative activity in Ohio and other Republican-led states. They further limited access to the pills, adding to restrictions on their use already in place in dozens of states around the nation.
“Over the past year, we’ve seen states really target medication abortion in a way that we hadn’t seen,” said Elizabeth Nash, state director for the Guttmacher Institute, an abortion rights group. “And so it’s particularly concerning because this is a method that is safe and effective and can be easily provided through telehealth.”
State prohibitions
This year alone, a half dozen states have passed laws targeting medication-induced abortion, according to Nash, and several others are advancing legislation. Arkansas, Arizona and Oklahoma enacted laws banning the mailing of mifepristone for abortions. Montana approved a measure effectively banning telehealth services for such abortions, as did Ohio, whose law is being challenged by Planned Parenthood in court.
Indiana passed legislation mandating that a patient take the first dose in the presence of a physician. The law also says abortion providers must tell patients that medication abortions can be reversed with progesterone — a claim the American College of Obstetricians and Gynecologists says is unsupported by science. That law is also being challenged by Planned Parenthood and other advocacy groups
The Texas Legislature, which passed a fetal “heartbeat bill” in May, is now expected to consider a bill to limit medication abortions once it reconvenes with a quorum for its special session. That measure also would ban the mailing of abortion pills and require doctors to examine a woman in person and ensure she’s no more than seven weeks pregnant before prescribing the medication.
Some of the recently passed measures also require women seeking medication abortions to receive pregnancy tests, ultrasounds and counseling. Meanwhile, about 20 states have laws preventing telehealth appointments for abortion pill prescriptions, and more than 30 restrict the health care providers who can write them, requiring they be doctors rather than physician assistants or nurses.
Oklahoma state Sen. Julie Daniels, who authored the medical abortion legislation, said at the time that the FDA’s moves to relax requirements for the pills prompted her to act. In addition to banning the mailing of abortion pills, the legislation would require a health care provider to handle any medical complications from their use and direct the state to develop certification requirements to prescribe the drugs.
“The abortion industry is pushing the federal government to abandon those safeguards and for the FDA to cease to monitor or regulate the use within the state,” she said. “So we’re scrambling to put together a regulatory framework so we in Oklahoma can track the use of these drugs, make sure they’re used appropriately and track any complications of the women who use them.”
The Susan B. Anthony List, an anti-abortion group, has been working with Republicans at the state level to craft these laws. Sue Liebel, the group’s state policy director, said that her organization has been monitoring the “meteoric rise” of what she termed “chemical abortions.”
“The pandemic itself gave the abortion industry an opportunity to try to move into that telemedicine space, and that’s where we’ve really been on the offense and the defense ever since,” she said. “States are also very aware that the FDA is looking to remove some restrictions that may actually cause the states to have to pick up the pieces.”
Liebel and other anti-abortion activists contend that mifepristone is not safe for women to take unsupervised at home and argue that it’s led to many rushing to emergency rooms. But of nearly 4 million women who have taken the drug since 2000, the FDA said, there were reports of 24 associated deaths as of 2018, including two cases of ectopic pregnancy and several cases of severe sepsis. Those deaths, however, could not be causally linked to the drug with certainty because of the patients’ use of other drugs or receipt of medical or surgical treatments, or their co-existing medical conditions and information gaps about their health status, the agency said.
Meanwhile, Planned Parenthood offers abortion pills through telehealth appointments in about 20 heavily Democratic states where it’s legal to do so and says there’s no medical reason to require prescriptions be given in person.
FDA weighing decision
Under the Biden administration, the FDA is reviewing whether to permanently lift the in-person dispensing requirement for the bills, which it could decide by December. But that move would have little impact on access for women in a huge swath of the nation because of the state-level statutory restrictions, advocates say.
“If a state law said that mifepristone must be dispensed and ingested in a physician’s office, then, you know, for all practical purposes, the FDA’s revised regulations would not make a difference for patients in those states,” said American Civil Liberties Union attorney Julia Kaye, who is involved in lawsuits challenging the FDA requirements.
In Missouri, which has just one remaining abortion clinic because laws targeting the procedure made it more challenging for providers to stay open, women have lost access to medication abortions.
Dr. Colleen McNicholas, chief medical officer of the clinic, Planned Parenthood of the St. Louis Region and Southwest Missouri, said that either women can get procedural abortions in her state or travel to Illinois, where abortion services are much more expansive.
Women who choose to get a procedural abortion in Missouri have to make two trips to the clinic — one for paperwork and the second for the abortion — which must be done at least 72 hours apart. So, most just make the 15-mile trip across the border to Illinois, where McNicholas operates another clinic, so they can get telemedicine appointments for abortion pills or whatever procedure they want done the same day, she said.
Dr. Colleen McNicholas, chief medical officer for Planned Parenthood of the St. Louis Region and Southwest Missouri.Reproductive Health Services of Planned Parenthood of the St. Louis Region
“Mifepristone is the only medication that they require you to receive in the clinic, but then you can self administer it at home. That doesn’t make any medical sense,” she said of the FDA requirements under review. “If it is safe for you to take it home, it should also be safe for you to receive it at home and then consume it at home.”
In January, Lee, the student in Ohio, moved to California because she transferred to a different college, and found out in June that she was pregnant again. She decided to get another abortion, again choosing the medication option. She felt more comfortable with the political environment in her new home than she did in Ohio, where anti-abortion advocates protested outside her clinic — and she was now more comfortable with the process.
“Obviously everyone’s situation is different,” she said. “I will say that, for me, it was good enough for me to do it twice. It was a very safe process.”
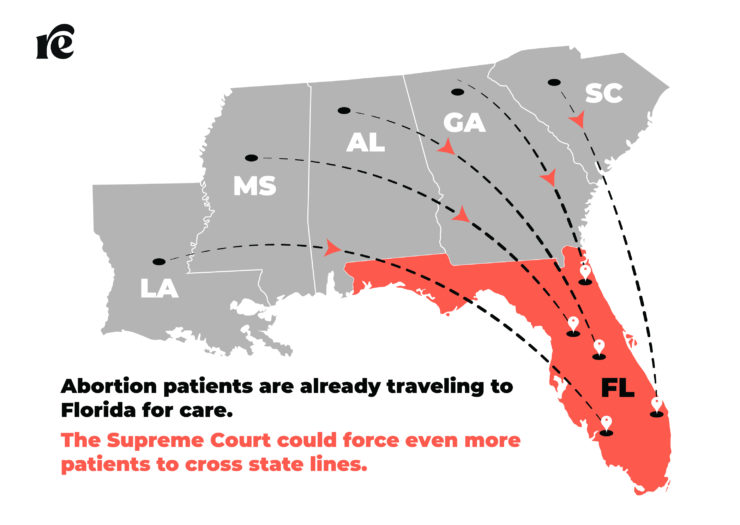
But what does that mean for people’s lives? If the Court sides with Mississippi here and allows states to ban abortion before fetal viability, it means even more people will have to cross state lines to get abortions than they do now.
Just how far will people have to travel to access what was once a constitutionally protected right?
For those living in the South, Florida seems like a safe haven. The “What if Roe Fell?” map from the Center for Reproductive Rights and a New York Times analysis suggest that, if the Supreme Court were to overturn Roe, abortion rights will be protected there and no clinics will close. Florida’s state supreme court recognizes the right to abortion under the state constitution’s right to privacy, plus there is no mandatory waiting period in effect and abortion isn’t restricted until 24 weeks of pregnancy.
But legally protected and accessible are not the same thing; Florida limits insurance coverage of abortion in both Affordable Care Act and Medicaid health plans, and minors need parental consent or a judicial bypass. And while Florida offers much more protection than any of the states it borders, with a Republican legislature and a governor considered to be a 2024 presidential contender, that could change. With a Supreme Court decision expected next June, people on the ground are preparing for whatever happens.
Even now, abortion patients travel into Florida for multiple reasons: The clinics may be closer, their home state restricts abortion after 20 or 22 weeks after the last menstrual period, or news reports about state legislation can lead people to think abortion is already banned in their state.
Shoring up resources
Clinics and abortion funds will do what they can to help people who may need to travel—that is, of course, if they can afford the trip.
Terry Sallas Merritt, who works in strategic management at A Woman’s Choice Inc., an independent clinic group with facilities in Florida and North Carolina, said people already travel from Georgia to the Jacksonville clinic in Northeast Florida, either because the clinic provides care up to 24 weeks or they simply want to avoid Georgia’s state-mandated waiting period.
After A Woman’s Choice saw an increase in patients who needed more financial and logistical help, it launched a patient support team in May 2020. The team helps people arrange everything from getting an appointment to securing money for the procedure, travel, food, or child care, as well as offering emotional support, Sallas Merritt said. A member of the team spends anywhere from two to seven hours assisting a patient who needs support.
Planned Parenthood has already expanded care in northern Florida due to increased demand. Laura Goodhue, vice president of public policy for Planned Parenthood of South, East and North Florida, said its Tallahassee center has seen a 30 percent increase in out-of-state patients in the last six months, while its Jacksonville clinic is also seeing more demand but with a less marked increase. Most people are traveling from Georgia, but there are also folks from Alabama, Louisiana, Mississippi, South Carolina, and even a few from Texas, Goodhue said.
To meet patients’ needs, the Planned Parenthood is increasing the number of days it provides abortion, adding evening hours, hiring more providers, and offering care up to 17 weeks and 6 days of pregnancy, an increase from 15 weeks and 6 days. Thanks to an anonymous grant, the affiliate also hired a patient navigator within the last year who helps patients coordinate out-of-state travel and lodging and assists people under 18 seeking judicial bypass so they can get an abortion without telling their parents. They’re looking into adding child care services at their health centers because they know that can be a huge barrier for patients, Goodhue said.
In a preview of what could come, the state’s other Planned Parenthood affiliate saw 20 to 30 patients from Texas during March and April of 2020 when abortion access flickered on and off, said Stephanie Fraim, president and CEO of Planned Parenthood of Southwest and Central Florida.“As long as the state holds strong with the laws we have right now, we can be someplace that women, particularly in the Southeast, can find sanctuary.” -Stephanie Fraim, Planned Parenthood of Southwest and Central Florida president and CEO
Fraim is prepared to increase capacity if her clinics see a surge in people traveling from out of state. The Orlando location offers abortion care four days a week, and Tampa offers five days. The Sarasota clinic, about an hour south of Tampa, currently offers abortions one day per week, but it could increase to two days. Some people fly into Orlando and drive southwest to Tampa or Sarasota because that’s where they have friends or family. (Fraim’s Orlando clinic also operates as an abortion care training center where providers-to-be from around the country spend anywhere from two to six weeks learning procedures, how to do medication abortions, patient education, and how to deal with protesters. But trainees can’t serve their communities if their state bans abortion.)
Unfortunately, one way clinics could ramp up abortion access is closed off in Florida: Thanks to an ultrasound and in-person consent requirement, patients are effectively unable to get medication abortion through telemedicine.
“It’s a shame—and a particular form of cruelty—that they don’t allow that to happen,” Fraim said. (Other pill options available in Florida include legally murky services like Aid Access and pharmacy sites.)
Fraim, who’s worked for Planned Parenthood for 17 years, has sometimes felt like Chicken Little shouting about what the Supreme Court could do to abortion access. But now that it’s taken a direct challenge to Roe, she is ready to activate her emergency network to help traveling patients with logistics like housing and car rides.
“I have a group of board members and donors and supporters who are well aware of what I’m going to be asking [of] them in the coming years,” Fraim said. “As long as the state holds strong with the laws we have right now, we can be someplace that women, particularly in the Southeast, can find sanctuary.”
An oasis of care in the South—but for how long?
It’s not clear that Florida’s laws will hold. Of the states in the South, Florida is the only one where abortion rights are considered “protected,” but it’s possible that could change in the next year, said Jennifer Driver, the senior director of reproductive rights at the State Innovation Exchange (SiX), a nonprofit that helps state lawmakers advance progressive policies.
“If you thought that 2021 in state houses was rough, 2022 could be just as bad with folks really sinking their teeth into what could come,” Driver said.
For evidence that Floridians can’t count on rights remaining as rights, they need only look to the 2018 referendum that restored voting rights to formerly incarcerated people—only for the legislature and Gov. Ron DeSantis to gut them, Driver said. “This idea that just because you’re ‘protected’ it stays protected, for Florida, makes me really concerned,” she said.
Driver thinks Virginia will take up Florida’s mantle of the South’s true safe haven, but traveling there may be just as far as Illinois for some people. “I mean, Virginia is what we call the South now,” she said. “But it makes me even more concerned because it’s just that much further from those true Southern states.”
Democratic state Rep. Anna Eskamani said Florida Republicans feel emboldened by the 2020 election, when Donald Trump won the state, and she suspects conservative lawmakers will push even harder now that there’s a direct challenge to Roe. (They also may want to shore up their anti-abortion credentials since 2022 is an election year.) Eskamani thinks Republicans may try a ballot initiative to rewrite the state constitution’s right to privacy in a way that would not protect abortion, though a similar effort failed in 2012.
“They’re going to try anything they can to water that down, to weaken it, so that Florida is not going to have a firewall in the face of a SCOTUS decision,” Eskamani said.
Eskamani also noted that an abortion ban in cases of fetal diagnosis—which she called “a clearly offensive piece of legislation”—passed the Florida House but not the senate last session, so it’s possible that effort could succeed in 2022. A ban on abortions after 20 weeks has been filed for at least the past three years but hasn’t gotten a vote so far. Plus, while the state’s 24-hour waiting period is temporarily enjoined, legal challenges are still pending and, if it were to go into effect, would present yet another barrier for patients. Eskamani and her colleagues will do what they can to fight these bills, including proposing amendments.
Newer kinds of challenges are also popping up. Goodhue said activists are trying to pass local ordinances banning abortion, attempting an end-run around the state constitution. Thus far they’ve succeeded in the Panhandle’s Santa Rosa County, which borders but does not include Pensacola.
The Florida Panhandle is relatively accessible for people traveling from southern Louisiana, Mississippi, and Alabama. But there is only one clinic in the Panhandle—in Pensacola—and it does not offer the standard of care for medication abortions. Rather than mifepristone and misoprostol, the clinic advertises a combination of methotrexate, a chemotherapy drug, and misoprostol, a regimen that causes more intense side effects. Many abortion funds don’t work with this clinic as a result.
The Florida Panhandle is a difficult area for abortion providers. Goodhue noted that the first known abortion provider to be murdered, Dr. David Gunn, was shot outside his Pensacola clinic in 1993, and the area is a hotbed of anti-abortion activity. She said Planned Parenthood doesn’t have plans to expand into the Panhandle at the moment; instead, it would focus on increasing capacity in Tallahassee, which is nearly 200 miles further east. It could put an already expensive trip out of reach for some people.
Mrs. K was a refugee who recently arrived in the U.S. to reunite with her husband and children. They arrived safely a few weeks ahead of her. On her initial refugee health exam, Mrs. K discovered she was six weeks pregnant. She had just arrived after escaping persecution in southeast Asia and faced the tremendous task of settling herself and her family in a new home. It was impossible for her to contemplate bringing another child into her family at the time. When Mrs. K came into the primary care clinic where I work seeking a medication abortion, I was happy to help her through the process.
In California, where my primary practice is located, any pregnancy-related care, including abortion care, is covered by Medicaid. Any person who is eligible for Medicaid and seeking an abortion for any reason can obtain the health care services they need without delay. That means access to an abortion as soon as someone decides, rather than having to delay for weeks to scrape together funds to pay out of pocket. The day Mrs. K. came into clinic, we signed her up for emergency Medicaid and provided her medication abortion that same day with full insurance coverage. She was able to quickly move forward to establish herself and her family in this new country, without having to worry about coming up with hundreds of dollars to pay out of pocket for the medication.
A counseling room is set up to receive patients.SCOTT OLSON/GETTY IMAGES
It’s a stark contrast to what my patients experience in Texas, where I regularly travel to provide abortion care. Texas has some of the most restrictive abortion laws, including banning state Medicaid coverage of abortion and even state-regulated private insurance coverage for abortion care. Unlike Mrs. K, my patients in Texas who have Medicaid coverage and private insurance alike have to fundraise—sometimes for weeks or months—in order to afford their abortion out-of-pocket. This burden was already heavy for people with Medicaid coverage who are struggling to make ends meet. It has been devastating in the midst of the COVID-19 pandemic when so many Americans had the rug pulled out from under them.
For the majority of people seeking an abortion in the U.S., obtaining an abortion is not as straightforward as it was for Mrs. K. The Hyde Amendment, inserted into every federal budget since 1976, prohibits federal insurance coverage of abortion care. Only 16 states allow state Medicaid funding to go toward coverage of abortion care. For those who have Medicaid insurance coverage in the other 34 states, paying for an abortion out of pocket is the only option available. This limitation in access to insurance coverage for an essential and constitutionally protected health care service leaves behind millions of people, based solely on their income levels and where they live.
What this means for my patients in Texas is that they might come into a clinic, undergo state-mandated counseling and unnecessary ultrasounds (additional barriers that Texas requires before obtaining an abortion), just to realize at the end of the day that they don’t have enough money to pay for their abortion. For some, the weeks of delay spent raising money may make it too late for a medication abortion, or they may need to delay an abortion into the second trimester with even higher costs. And this doesn’t account for the additional costs of travel and accommodations, child care and days off of work that many people face when obtaining an abortion. Each of these stacking costs and barriers at each step can be overwhelming and seem insurmountable for some families. The burden of this policy falls particularly on communities of color, who are disproportionately represented among Medicaid recipients, and who historically have had the most barriers in obtaining equitable health care.
The House recently took an important step by passing a spending bill without the Hyde Amendment for the first time in decades. The Senate must follow suit. This is a racial and economic justice issue just as much as it is a health care and reproductive justice issue. It’s unconscionable to continue discriminating against my patients based on their income level and where they live. Eliminating the Hyde Amendment and covering all pregnancy-related care, including abortion, is critical to achieve true reproductive justice and liberation.
Pro-choice activists supporting legal access to abortion protest during a demonstration outside the U.S. Supreme Court in Washington, D.C., March 4, 2020. (Saul Loeb/AFP/Getty Images/TNS)
WASHINGTON — The partisan fight over whether the federal government will fund abortion coverage for Medicaid beneficiaries threatens to stall action on major appropriations bills, but the on-the-ground impact would be less dramatic than the debate suggests.
Democrats are prioritizing the removal of an annual appropriations rider known as the Hyde Amendment, which bans federal funding of abortion except in cases of rape, incest or to protect the life of the woman. The policy, which prevents programs like Medicaid or the Children’s Health Insurance Program from using federal money to cover abortion outside of those three situations, has been in every spending law since 1976.
Additional legislative action outside of the fiscal 2022 Labor-HHS-Education funding bill would be needed to broaden abortion coverage for women who receive care through departments such as Defense or Veterans Affairs.
It would be challenging to remove a long-standing abortion policy that every lawmaker who voted for Labor-HHS-Education funding in previous years allowed to continue.
Even if changes to Hyde become law, the effects would be muted, based on state abortion policies, said Laurie Sobel, the Kaiser Family Foundation associate director for women’s health policy.
“It certainly would signal a change in federal policy in the willingness to fund abortions. But given that Medicaid is a federal-state program, there’s room for the states to make their own policies,” she said. “It wouldn’t change the policy across the country. What it would do would be to provide federal support for the states that choose to provide abortion services under their Medicaid program.”
Sobel said that unless abortion becomes required under Medicaid, states that oppose the policy could continue to exclude abortion as a benefit. Changing federal benefits is a complicated process.
Essentially, she said, if the Hyde amendment were to go away at the federal level without any benefit changes, then states that cover abortion could obtain a federal matching payment for those services. But states that do not want to cover abortion would not have to do so.
“The only real impact would be that the states that include abortion currently would be able to pull down the federal match,” she said.
Data on how many abortions are currently covered by federal funding under the three exceptions is limited.
A 2019 Government Accountability Office report, using state-reported numbers, said the average number of abortions eligible for federal funding per year between 2013 and 2017 was about 1,339 or fewer.
But the number acknowledges various gaps in data, including for several states and for services covered by managed care.
Separate data from 2014 shows that in states that follow Hyde restrictions, Medicaid covered only 1.5% of abortions.
“There’s very few cases of Medicaid paying for abortion in the Hyde states. Even for the cases of rape, incest and life endangerment, it’s very few abortions being paid for because you have to jump through a whole bunch of hoops to get it covered,” said Sobel.
Meanwhile, the overall number of abortions performed in the United States has been falling.
Still, the fight over abortion restrictions will likely be a major flashpoint in appropriations debates and on the campaign trail. The House is expected to vote next week on a package of seven fiscal 2022 spending bills that will omit the Hyde limits. It’s unlikely that Republicans will sign on without the restrictions.
Democrats say repealing the Hyde Amendment would remove barriers for low-income women and women of color who are disproportionately affected by the ban.
But Republicans say the Hyde Amendment protects the rights of taxpayers who oppose abortion and has increased the nation’s birth rate.
States can use their own funding to provide abortion coverage for Medicaid and CHIP outside of the three Hyde Amendment exceptions, but only 16 do, including Illinois, Maryland and New York.
California is the most populous state that covers abortion broadly. Enrollees don’t pay out-of-pocket costs or have to give medical justification.
Without Hyde limits, the biggest changes might be seen in left-leaning states, like Colorado or Delaware, that currently do not cover most abortions under Medicaid except for the three allowed circumstances.The Columbian is becoming a rare example of a news organization with local, family ownership. Subscribe today to support local journalism and help us to build a stronger community.Subscribe Today
Thirty-three states and the District of Columbia do not cover abortion except under the three Hyde exceptions for individuals with federal coverage. Additionally, South Dakota, the only state with abortion funding restrictions more restrictive than Hyde, covers abortion under Medicaid only when necessary to protect the life of the woman.
The Guttmacher Institute, which supports abortion rights, estimates that 7.8 million women of reproductive age are covered by Medicaid in these 34 states and D.C., and half of them are women of color.
Elizabeth Nash, interim associate director of state issues at the Guttmacher Institute, said any changes to allow more abortion funding would not have an immediate effect.
For instance, abortion providers would only be paid if they are Medicaid providers. Nash said state officials who oppose abortion could make it harder for providers to become Medicaid providers or increase red tape.
“I really do think that the lag time will unfortunately be an issue,” she said.
Guttmacher national data also shows that among women of reproductive age, 29% of Black women and 25% of Hispanic women had Medicaid coverage in 2019. That number drops to 15% for white women and 12% for Asian women.
Researchers at the Advancing New Standards in Reproductive Health, or ANSIRH, program within the University of California, San Francisco’s Bixby Center for Global Reproductive Health conducted a national study of individuals who were searching online for abortions.
The April study found that residents of states that do not have broad Medicaid coverage of abortion faced more financial barriers and spent more time seeking an abortion. It found Black and Latina women were more likely than white and Asian women to still be pregnant and seeking an abortion when followed up with four weeks later.
“These findings indicate that restoring federal Medicaid coverage of abortion by repealing the Hyde Amendment would remove an often insurmountable barrier to abortion care for low-income people,” the researchers wrote.
ANSIRH data from a 2018 report showed that women who end up giving birth instead of getting a wanted abortion saw an almost fourfold increase in the odds that their household income was below the federal poverty level.
Kaiser Family Foundation data suggests that if abortion coverage were available across Medicaid, more women would have abortions. But the number of Medicaid-funded abortions would depend on factors like the number and availability of local abortion providers, state-level restrictions on abortion, income demographics and local reimbursement rates.
For some low-income women, not having coverage of abortion serves as a de facto ban.
A 2019 peer-reviewed study in BMC Women’s Health showed that in Louisiana, 29% of pregnant women who qualify for Medicaid would have had an abortion if it were covered.
Destiny Lopez, co-president of All Above All, which supports repealing the Hyde Amendment, called abortion access in the U.S. “a patchwork and a puzzle.”
“You have created an unfair and unjust system because women with means will always be able to get an abortion in this country,” Lopez said.
Hyde Amendment supporters see it differently.
Michael New, a research associate of political science and social research at The Catholic University of America and Charlotte Lozier Institute associate scholar, does not want Hyde removed.
The Charlotte Lozier Institute, the research arm of the conservative Susan B. Anthony List, estimates that the Hyde Amendment resulted in 2,409,311 births from 1976 to 2020.
“I think that researchers, both pro-life and researchers who support legal abortion, pretty much all agree that the Hyde Amendment lowers the abortion rate and saves lives,” he said.
He disagrees that Hyde singles out certain people.
“Hyde is a policy that encourages women to seek life-affirming alternatives like pregnancy help centers and other resources for support. I don’t think Hyde is targeting people. I think it’s protecting people,” New said.
The fight over the Hyde Amendment is just beginning. The House Appropriations Committee advanced its fiscal 2022 Labor-HHS-Education spending bill on July 15, with all Republicans voting against the measure.
“It’s my hope that members on both sides of the aisle and in both chambers can negotiate spending that is responsible and will not lead to financial disaster. But the first step toward negotiation is the full reinstatement of the Hyde Amendment,” said House Labor-HHS-Education Appropriations ranking member Tom Cole, R-Okla., who offered an amendment during the markup to restore Hyde language into the bill.
It was rejected, with only one Democrat, Henry Cuellar of Texas, voting for it.
Senate Republicans already said they won’t support a spending bill without Hyde language.
Sen. Mike Braun, R-Ind., an appropriator, went to the House markup to show his support for the language. Senate Minority Leader Mitch McConnell also spoke on the Senate floor last week in favor of Hyde limits.
Republican opposition to changing this policy has not stopped Democrats from moving forward, which has the blessing of President Joe Biden. Biden had supported Hyde before announcing in 2019 he had changed his stance.
Insurers sometimes don’t cover certain contraceptive methods for free, though they are supposed to cover most by law. Even for long-established methods, like IUDs, insurers sometimes make it hard for women to get coverage by requiring preapproval. BSIP/Universal Images Group via Getty Images
For Stephanie Force, finding a birth control method that she likes and can get without paying out of pocket has been a struggle, despite the Affordable Care Act’s promise of free contraceptives for women and adolescent girls in most health plans.
The 27-year-old physician recruiter in Roanoke, Va., was perfectly happy with the NuvaRing, a flexible vaginal ring that women insert monthly to release hormones to prevent pregnancy. But her insurer, Anthem, stopped covering the branded product and switched her to a generic version in early 2020. Force says the new product left her with headaches and feeling irritable and short-tempered.
After talking to her OB-GYN, Force tried an IUD. But that made her feel worse: She had bad cramps, gained 10 pounds and developed severe hormonal acne. Plus, she was charged $248 for an ultrasound her provider used to guide the insertion of the device, a charge she successfully fought.
Force also considered a couple of birth control products approved in recent years: a non-hormonal vaginal gel called Phexxi and a vaginal ring called Annovera that can be used for a year. But Phexxi isn’t covered by her employer health plan, and she would owe a $45 copayment for Annovera.Article continues after sponsor message
Despite the Affordable Care Act’s guarantees for free contraception coverage, Force’s experience illustrates that even for women whose health plans are subject to the law’s requirements, obtaining the right product at no cost can be onerous. New types of contraceptives aren’t automatically incorporated into the federal list of required methods that insurers use to guide coverage decisions.
In addition, some health plans continue to discourage use of even long-established methods, like IUDs, by requiring providers to get approval from the plan before prescribing them.
Consumer advocates who have studied the issue say a process is spelled out in federal rules for women to get the contraceptives they need, but far too few people know that’s an option. (For more on how to do this, see the final section below.)
Ultimately, Force went back to the generic version of the NuvaRing, despite the side effects she continues to experience. She’d prefer to be on the branded NuvaRing, which didn’t give her problems, and the ping-ponging from method to method has left her exhausted and furious.
“I cannot believe what hoops I have had to jump through between September 2020 and June 2021,” Force says, “between switching from the generic NuvaRing to the IUD and then back, fighting my insurance and OB-GYN’s office on the ultrasound charge.”
In a statement, Anthem says, “Anthem health plans cover 222 contraceptive products at $0 cost share on our ACA Preventive List.” The company went on to say that it covers “at least one product” in each of 18 categories of contraception methods approved by the FDA.
A policy meant to cut contraceptives’ costs
Contraception is a very personal choice, and what meets one woman’s needs may not meet another’s. If avoiding pregnancy is a woman’s top priority, a virtually fail-safe method like an IUD may be the right solution. But for someone who’s considering getting pregnant soon, a readily reversible method like a birth control pill might be the best option. Side effects are important to consider as well, since women respond differently to the hormones in various birth control products.
Before the Affordable Care Act (ACA) required no-cost birth control coverage, researchers estimate that up to 44% of women’s out-of-pocket health care spending went toward contraceptives. The ACA requires most commercial health plans to cover a comprehensive list of Food and Drug Administration-approved methods without charging women anything.
Church plans and religious nonprofits, as well as employers and schools that object to contraception, are exempt from the coverage requirements. Plans that were grandfathered under the law are also exempt. Uninsured women don’t benefit from the mandate either.
But the federal rules do not require health plans to cover every single contraceptive. After the ACA passed in 2010, the federal Health Resources & Services Administration (HRSA) developed guidelines for women’s preventive services.
Those guidelines say women should have access without cost sharing to a list that covers the 18 FDA-approved methods, including oral contraceptives, vaginal rings, cervical caps, IUDs, implantable rods and sterilization. Under federal rules, health plans must cover at least one product in each category.
New products are left out
Neither the HRSA guidelines nor a birth control chart published by the FDA addresses newer methods, including Phexxi, a gel that regulates vaginal acidity to reduce the odds a sperm reaches an egg. It was approved by the FDA last year.
“There’s a real need for new guidance that keeps up with new methods,” says Mara Gandal-Powers, director of birth control access at the National Women’s Law Center.
Many insurers have balked at covering Phexxi, says Rameshwari Gupta, director of strategic markets for Evofem Biosciences, which markets Phexxi. A box of 12 single-use applicators — consumers use one before having sex — costs $267.50 without insurance, she says.
“When I started talking to payers, they all said, ‘Where are you on this FDA chart?’ ” she says.
According to an FDA spokesperson, the birth control chart is for consumer education purposes only and “was not created with the intent of driving coverage decisions.” The agency is in the process of updating it.
In a statement, the HRSA says it is reviewing the evidence on contraceptives and expects to complete its review late this year. If it opts to make revisions, it will publish draft recommendations to update the women’s preventive services guidelines. These will be finalized after a public comment period and become effective a year later.
At this point, health plans consider Phexxi to be a spermicide and are required to cover only one type of spermicide without cost sharing, says Kristine Grow, a senior vice president at AHIP, a health insurance trade organization.
“If Phexxi is indeed considered a new method of contraception, both the FDA and HRSA would need to make this clear,” she added.
Cost sharing and preapprovals limit access to some methods
The vaginal ring Annovera, approved by the FDA in 2018, is typically covered by health plans, according to Grow, though it may not be available without cost sharing. The average retail price is $2,457 a year, according to GoodRx.
One way plans have made it difficult for women to access certain contraceptives, even those on the list of approved methods, is by requiring that their providers get approval from the insurer first, often by providing documentation that the product is medically necessary.
Under UnitedHealthcare’s coverage policy for Phexxi, for example, before coverage will be authorized, members must have documented reasons that they are unable to use eight other contraceptive methods, including oral contraceptives, the contraceptive patch, a vaginal ring, injections and spermicides. Providers also must attest that they have counseled patients that Phexxi is less effective at preventing pregnancy than some other methods.
In a statement, UnitedHealthcare says it covers “a broad array” of generic and brand-name options, and it follows scientific evidence to develop its list.
Yet consumers have a way to get the specific method that is most appropriate for them, according to a report by the National Women’s Law Center.
How to get a birth control method covered
Under federal rules, if a doctor or other health care provider determines that a patient needs a particular contraceptive, even if it’s not on the list of approved products for the patient’s plan, the insurer is required to have an expedient process for the patient to seek a waiver.
“It’s not up to the insurance company whether to cover that method — it’s up to the provider,” says Adam Sonfield, executive editor for policy analysis at the Guttmacher Institute, a research and advocacy organization focused on women’s reproductive health.
But according to the National Women’s Law Center report, many insurers, patients and their providers aren’t aware of the requirement, and state agencies don’t enforce these so-called exceptions policies.
If patients run into trouble getting the method they want, “we typically recommend filing an appeal with their insurance provider,” says Gretchen Borchelt, vice president for reproductive rights and health at the National Women’s Law Center.
Stephanie Force says she was unaware of any process she could have used to get the NuvaRing covered without cost sharing. Neither her health care provider nor the insurer mentioned the possibility.
She recently had an appointment with a new provider who she hopes will be a better advocate for her.
Protesters rally against a bill outlawing abortions after a fetal heartbeat is detected outside the Texas Capitol on May 29 in Austin.Sergio Flores / Getty Images file
Abortion advocates in Texas say the law will encourage their opponents to flood courts with lawsuits that will cripple their ability to operate.
For Anna Rupani, harassment comes with the job.
As the co-executive director at Fund Texas Choice — a practical-support abortion fund in Texas that helps women travel to places, both in and out of the state, where they can receive abortion care — she’s been the target of protests, violent threats, online bullying and terrifying mail.
But should a novel law in her state go into effect Sept. 1, those who oppose her work will be able to express themselves through the courts — with the likely practical effect of suing her fund and others like it into oblivion.
That law, known as S.B. 8, bans abortions in Texas as early as six weeks into pregnancy — before many women even know they are pregnant. But unlike every other anti-abortion law, Texas’ unique ban will be enforced through private citizens’ lawsuits, rather than through state government. It includes first-of-its-kind language that allows anyone, even someone outside Texas, to sue an abortion provider or anyone else who helped someone get an abortion after the six-week limit for at least $10,000 per defendant.
“This is basically all to create a chilling effect. Even if these lawsuits are thrown out, organizations like ours will have to keep defending themselves in court every time,” Rupani said. “It’s all about putting us out of business.”
Targets could include not only abortion funds and practical support organizations that provide women in need with money, transportation, lodging, recovery care and child care, but also doctors, nurses, domestic violence counselors and even friends, parents, spouses and clergy members who drive a woman to a clinic or even just provide counseling about whether to have the procedure. Abortion-rights groups have filed a suit in federal court seeking to block the law from going into effect.
Abortion-rights advocates in Texas say the law will encourage their opponents to flood courts with lawsuits that will cripple their ability to operate — their limited time and resources spent on fighting suits instead of care and support. If that happens, women will be isolated from the little support available to them during these vulnerable moments. In interviews, they called the law “insidious,” “draconian,” “cruel” and “pernicious.”
Experts who study and track abortion access, however, said the law is actually the embodiment of a broader, more extreme and increasingly aggressive wave of vigilantism that, at least in the anti-abortion movement, began with protests and sporadic acts of violence. The threat then moved online, they said, and now, in Texas at least, it has moved to the courts, where abortion foes will be empowered to hunt for financial bounties by suing their opponents.
Elizabeth Nash, a state policy analyst at the Guttmacher Institute, a research organization that studies reproductive health rights, said one of the law’s most concerning pieces is that its enforcement was in the hands of individuals, not law enforcement, eager to shut down and harass abortion clinics and support providers.
“It literally provides a financial incentive for the kind of harassment and vigilantism we’ve seen grow decade after decade,” she said.
Legal experts said that if the law is upheld, anti-abortion activists will face an uphill battle proving in court that other people’s abortions are personally injurious to them, the typical hurdle for allowing this kind of a lawsuit to advance in court. Still, it will nevertheless bring mischief for abortion care advocates, legal experts said, by inviting frivolous lawsuits that abortion supporters will have to pay to defend against, even if they win every single one.
“It’s the legalization of harassment without holding the government liable,” Rupani said.
Meanwhile, Texas Gov. Greg Abbott, a Republican, has lauded the bill as a measure that “ensures that the life of every unborn child who has a heartbeat will be saved from the ravages of abortion.” Its author, Republican state Sen. Bryan Hughes, has frequently spoken of his belief that the bill will more effectively stand up to legal challenges than previous ones that relied on law enforcement, and at least one prominent anti-abortion group, Right to Life East Texas, has vowed to begin suing individuals under the law as soon as it goes into effect.
‘It’s bounty hunting’
S.B. 8 doesn’t outright criminalize abortions after six weeks, but rather encourages civil lawsuits at the municipal, county and state level targeting the process by which a woman might seek abortion care.
The law is also uniquely designed to disadvantage defendants, experts said. All damages would go right into the plaintiff’s pocket. If a defendant wins, they still must pay their own legal fees, but if a plaintiff bringing a suit wins, the defendant must pay both sides’ legal fees. Individuals who are thought to be helping a woman obtain abortion care can be sued multiple times by different people and parties.
“It bakes in incentives and takes away disincentives for vigilante enforcement,” said Adriana Piñon, a senior staff attorney and policy counsel with the American Civil Liberties Union of Texas.
“It’s bounty hunting,” added the Rev. Katherine Ragsdale, president of the National Abortion Federation. “Abusive spouses, disapproving parents, angry neighbors or people with no relation at all will all have a legal right to harass,” she said, before connecting it to a broader rise in extremism in recent years.
“This kind incentivized vigilantism isn’t just about abortion issues. It’s private individuals patrolling the border with guns; it’s insurrectionists storming the U.S. Capitol. Now it’s the ability to sue about helping with or providing abortion care,” she said. “It’s part of a growing level and climate of vigilantism and violence that large chunks of the country feel is justified.”
‘A new and frightening chapter’
The use of aggressive tactics against abortion-rights groups is nothing new. But the prevalence and intensity of those tactics have grown in recent years.
According to NAF’s latest violence and disruption report, acts of violence and disruption targeting abortion providers — including invasions, trespassing, assault and battery, death threats and threats of harm, hate mail, hate calls, hate emails and bomb threats — rose 22 percent to more than 153,000 incidents in 2019 (the most recent year NAF has assessed), an all-time high, the majority of which were incidents of picketing.
Multiple officials at abortion funds and abortion clinics described a huge uptick in hacking and online bullying in recent years, too.
That includes Amy Hagstrom Miller, CEO of Whole Woman’s Health, a network of abortion clinics across Texas, and a plaintiff in a federal lawsuit to block S.B. 8 from going into effect, who said her group has seen hundreds of attempts by hackers to take her group’s site down and access her group’s databases.
But because of S.B. 8, she and numerous others said, the venue for that kind of intimidation would now be the U.S. court system.
“It’s the unusual next venue for that kind of surveillance and harassment and intimidation that anti-abortion folks have engaged against clinics and patients for decades,” she said.
“But it’s nonetheless yet another new and frightening chapter, because it’s formalized the ability for the anti-abortion movement to have a private cause of action against clinics and people helping others get to the clinic,” she added.
Lawyers working on the suit to block the law from going into effect have expressed cautious optimism about their case, even though they are challenging a law that was cleverly designed with a new, untested enforcement mechanism in mind.
“We don’t think Texas’ strategy is going to be successful because, even though private individuals are enabled to file suits, ultimately there are still government officials in charge of enforcement of the law. It’s just that these officials are in the court system, not law enforcement,” said Marc Hearron, who as senior counsel at the Center for Reproductive Rights is working on the suit.
But abortion-rights advocates say that doesn’t matter: If the law is upheld, the avalanche of lawsuits still means just about anyone who opposes abortion could use the court system to stop people like Zaena Zamora, who runs the Frontera Fund, which provides money for care and travel. As a result, Zamora could be sued by countless people for each woman she has helped receive abortion care.
Last year, Zamora helped about 400 women who live in the southern-most tip of Texas, predominantly Hispanic and below the poverty line, travel within and outside of the state to receive care. That would amount to a minimum of $4 million in damages owed, plus legal fees for both sides in each suit. Zamora’s yearly budget for practical support and abortion care funds is below $100,000.
“It would bury us in litigation and bills that would undoubtedly stop us from doing the work we do,” Zamora said. “Imagine being able to pocket $10,000 for harassing a group like ours. The cruelty is the point.”