“There’s a real disconnect between the reality of the way most Americans feel about abortion and what we do see reported and what has emerged as the prevailing narrative, which is that abortion is a divisive issue. It’s not a divisive issue,” said Rewire News Group President and Editor-in-Chief Galina Espinoza. Alex Wong/Getty Images
Despite the majority of people supporting abortion, the topic is still described as a polarizing issue.
Earlier this month, Rewire News Group President and Editor-in-Chief Galina Espinoza and Senior Editor, Law and Policy Imani Gandy joined the University of Pennsylvania’s Sophie Maddocks in a conversation about the future of reproductive justice under the Biden administration. What can the public discourse on sex discrimination and reproductive rights tell us about the health of democracy?
A brief transcript follows below. Watch the full conversation here.
Sophie Maddocks: I think it’s so alarming to hear about this complete misinformation/disinformation and that’s been propagated for so long. … What role has the mainstream media played in colluding with this and in polarizing the abortion debate? And how has this developed under the Trump administration as well?
Galina Espinoza: I’m so glad to hear you use the word polarizing because it gives me the opportunity to debunk one of my favorite myths, which is that abortion is a polarizing issue. It’s completely reasonable that most folks think that abortion is a polarizing issue based on the way that it is reported in the mainstream media.
But here are the facts. The facts are that 70 percent of Americans believe that abortion should be legal most or all of the time. I would challenge you to find any other issue in America right now that 70 precent of folks agree on. I mean, it’s a really clear majority, even when you start to look at people of faith, which is a conversation that’s come up a lot since the election of President Biden as a Catholic president. The Pew Research Center last year did a poll of Catholics and more than half of them also believe that abortion should be legal in most or all cases.
There’s a real disconnect between the reality of the way most Americans feel about abortion and what we do see reported and what has emerged as the prevailing narrative, which is that abortion is a divisive issue. It’s not a divisive issue.
Imani Gandy: When you talk about the polarizing nature of abortion, you’re usually talking about certain kinds of abortion. The anti-choicers love to focus on later abortion, which is about 1.2 percent of the abortions that people have. They like to focus on these later abortions, because it tugs at the heartstrings, the idea of a 28-week pregnant person deciding just willy-nilly that they “just don’t want to be pregnant anymore … just kidding I’m going to have an abortion,” which is not something that happens.
What I find really interesting is thinking about the ways in which questions regarding abortion are posed. When you are polling people about their feelings about abortion, the way you phrase the question can really change the outcome and can change the answer. For example, there are six-week bans, these “heartbeat bans.” Well, first of all, embryos don’t have heartbeats, they don’t have cardiovascular systems. So right out of the gate that’s a way that the media is sort of cementing this anti-choice narrative about heartbeat bans.
But besides that, if you were to ask a person, do you think that abortion should be permitted after a fetus has a heartbeat? People might say, well, no, because then they’re getting really close to [becoming] a person and that just seems icky. But if you explain to them that there is no cardiovascular system, that fetuses and embryos do not have heartbeats and then you say, well, what if I told you that banning abortion at six weeks means that most people won’t be able to get an abortion, because most people don’t know that they are pregnant at six weeks, so it’s basically a total abortion ban. You’re foreclosing that option for a lot of people. Well, the answer is going to change.
Watch the full conversation below. A transcript is available here.
Lockdown revolutionised women’s access to home treatment – and strengthened the anti-abortion backlashby Sarah Hurtes and Daniel BoffeyWed 21 Apr 2021 08.00 BST
Kay, 34, realised her period was late a month into Britain’s lockdown. The coronavirus death count was spiralling across the country. Covid-19 was putting the NHS under unprecedented strain and Boris Johnson had given the British people what he described as “a very simple instruction” in an address to the nation from Downing Street: “You must stay at home.”
A worrying, unsettling time, and Kay, a mother of a six-year-old girl, needed to get hold of a pregnancy test kit. She went online and, two days later, took delivery of the test, learning of a positive result via two pink lines. It was the news she had dreaded.
“I had always hoped to have a large family but with a list of health complications during my first pregnancy and a scar across my tummy to remind me of the ordeal, I was sure that I could not physically or mentally manage to carry a healthy pregnancy,” Kay said. She took the agonising decision to have an abortion. But how?
Across Europe in spring 2020, as the pandemic was closing down everyday life, so too were the shutters falling on “non-essential” health services. Drastic decisions were being made by rattled European authorities. In countries where abortion was already a highly contested right and wherepowerful and vocal anti-abortion lobby groups were on high alert, governments swiftly jumped towards restrictions.
Abortions would be banned in six countries – Andorra, Liechtenstein, Malta, Monaco, San Marino and Poland – according to a 46-nation survey published in the British Medical Journal. Surgical abortion was made less available in a further 12 countries and in 11 countries, services were made unavailable or delayed for women with Covid-19 symptoms.
Abortion became “probably one of the most endangered rights in Europe”, said David Paternotte, a researcher at the Université Libre de Bruxelles.
Kay was fortunate in one respect during this troubling, emotionally fraught time. The UK was going another way.
As some European countries restricted abortion, others took a quite different approach, innovating to minimise in-person consultations in a way that some experts believe could permanently change the face of abortion rights.
As the likes of Poland slammed doors shut on women, regulatory barriers to abortion have been lifted to varying degrees in 12 countries – Belgium, Estonia, Ireland, Finland, France, Norway, Portugal, Switzerland, England, Wales, Scotland and Northern Ireland.
A protest in Warsaw against the Polish constitutional court’s ruling restricting abortion rights. Photograph: Kacper Pempel/Reuters
This liberalisation is “one of the few really positive things to come out of the pandemic”, said Jonathan Lord, a consultant gynaecologist for the NHS and medical director at MSI Reproductive Choices, formerly known as Marie Stopes International, one of the country’s four abortion providers. “It has empowered us to improve the whole [abortion] care pathway almost overnight,” he said. It offered hope to others.Advertisement
At the same time, the voices of the Christian right have grown louder and some sympathetic governments have been emboldened to heed their calls. After interviews with women affected, policymakers, activists, lawyers, and providers, this is the story of how the pandemic has widened the inequities in abortion rights across Europe.
While the pandemic response in Britain and a handful of othernations has offered the future potential for more equality in access to treatment and care for women there are also signs of a worrying backlash, say campaign groups. Progressive policy developments in the UK and elsewhere have been seized on by anti-abortion campaigners as evidence of a need to bolt down the doors.
‘Telemed’ abortions
On the evening of 30 March 2020, with the UK in full lockdown and abortion services at risk of collapse, the Department of Health and Social Care in Whitehall published a new policy. Women in England would be able, at least temporarily and after a phone or video consultation with a doctor, to take prescribed abortion pills at home, removing the need to travel to a clinic. The Scottish and Welsh health departments followed suit the next day.
Medical abortions, via pills administered before 10 weeks, account for the vast majority of abortions in the UK. They take place in two stages. Before the coronavirus outbreak, women were legally obliged to take the first pill, mifepristone, at a clinic. The second pill, misoprostol, which taken up to 48 hours later, triggers miscarriage within hours and is usually taken at home – although even that is a recent reform. Until 2018, women in England had to also take both the first and the second pill at a clinic, with the risk that their pregnancy could end in a taxi or on public transport as they travelled home.Advertisement
The pandemic-led shift to full “telemed abortion” did not come out of nowhere. According to Lord, its advantages had been known for years, and it was included in a “blueprint” for the NHS in England that was published as part of the National Institute for Health and Care Excellence (Nice) guidelines in September 2019.
“Normally there would have been a protracted phase of planning, and then evaluation, and people getting cold feet,” Lord said. “Moving forward, probably, you’re looking at three to five years of getting it embedded.” Then Covid-19 hit, and instead of the lengthy delay Lord had anticipated, the nation’s medical sector realised very quickly that abortion care was “exceptionally vulnerable and totally time-limited”.
A few other countries were of a like mind. In France and Ireland, the gestational limit of medical abortion at home was raised to nine weeks and the usual mandatory in-person consultation was dispensed with. In Francophone Belgium, although not Dutch-speaking Flanders, abortion centres started promoting medical abortion up to eight weeks at home with phone supervision.
Abortion became probably one of the most endangered rights in Europe
David Paternotte
For Kay, the new law was a huge relief. “I am ashamed to say I had always been very anti-abortion during my younger years, however, now older and wiser, I researched my options and found out about telemedicine,” she said.
On a chilly morning in May last year, Kay took the first pill and got on with her day. After 12 hours she had a night fever, sweating and shivering. It was short-lived. She went back to sleep and awoke the next day to take the second round of pills. “I was really scared about the possible side-effects, but a lovely nurse on the end of the helpline reassured me and suggested I inserted the pills vaginally for less risk of side-effects.”
After four and a half hours, Kay began to pass the pregnancy. No pain, no side-effects, and no different for her than a regular period. Three weeks later, she took the special pregnancy test that came with the pills to ensure the process had ended the pregnancy – and indeed it had.
According to Lord, more than 70,000 women in England will have had telemedicine abortion in the year since it was introduced. There were no cases of women having a severe infection or needing major surgery, Lord said. “The rate of inadvertent late gestation was 0.04%, and all these still had a safe and successful abortion.” Additionally,data from the British Pregnancy Advisory Service shows that since the introduction of telemedicine, almost 50% of abortions were performed before seven weeks gestation from January to June 2020, compared with nearly 40% for the same period in 2019. Waiting times for women seeking abortion care have more than halved.Advertisement
Kay and others were fortunate to have the treatment they needed when they needed it. It would prove to be more than thousands of women elsewhere in Europe could possibly hope for.
Women ‘trapped in hospitals’
Braving freezing January temperatures and the batons of riot police, thousands of women across Poland marched through the streets. “My government is killing me”, “My body, my choice” and “The revolution has a uterus” were some of the placards waved by the crowds.
Strongly Catholic and governed by rightwing social conservatives, Poland has some of the most restrictive abortion legislation in Europe. Before the pandemic, abortions had been permitted only where there was a threat to the mother’s life, a foetal abnormality, or where pregnancy had resulted from rape or incest. But in October 2020, Poland’s constitutional tribunal issued a ruling that ended the possibility of legal terminations in cases of foetal abnormality. Almost all abortions had been carried out on those grounds before the ruling. The new law’s entry into force felt like a moment of deep fear for many, campaigners said.
Protesters on the streets of Warsaw after the imposition of a near-total ban on abortion in January. Photograph: Justyna Rojek/East News/Rex/Shutterstock
Krystyna Kacpura, of the Federation for Women and Family Planning (Federa), said women were left “trapped in hospitals” waiting for the intervention or even right in the middle of the procedure when the government decided to formally enact the ban on 27 January. Kacpura received appeals from “desperate women, husbands and doctors the whole night,” she said. It had been an ongoing nightmare since then, she said.
“Just last month there was a woman who had a therapeutic abortion scheduled because the foetus did not have a brain,” Kacpura said. “We helped her getting the first certificate from a psychiatric specialist, but at the hospital they demanded a second opinion, and that’s when the woman threatened to end her life.”
Those who support the government’s move say the balance in the law needed to be corrected. “An unborn child is a separate person, which has its own body and its own rights. A child must not be deprived of the fundamental right of every human being – the right to life,” Kaja Godek, one of Poland’s most prominent anti-abortion campaigners, wrote on Facebook.
The move has led to a wider reckoning, too. In light of the constitutional court’s ruling, the anti-abortion Fundacja Pro Prawo do Życia in Poland asked the public prosecutor to investigate all abortions carried out after 22 October 2020. According to members of Federa, prosecutors are going through hospital records in eastern Poland. The organisation says it has also received a large volume of calls from people who ordered medication for self-managed abortion and have been summoned to make statements at police stations.
An abortion rights protester during a demonstration in Warsaw. Photograph: Attila Husejnow/SOPA Images/REX/Shutterstock
“You can imagine what impact such investigations can have on doctors or people assisting in abortion in the whole of Poland,” said Kacpura.
Where Poland has gone, others are in danger of following, campaigners say. In Hungary, where again the abortion law with its mandatory counselling and waiting periods had been a point of criticism before the pandemic, a conservative lobby group, CitizenGo, has been campaigning for a suspension of abortion services. Amnesty International has said it fears there will be a knock-on effect in Bulgaria, Slovakia, Belarus and Romania.
Even countries potentially minded to liberalise rather than restrict during the pandemic have been put under pressure through the courts not to follow the lead of the UK, France and Ireland.
In Spain, where the government is consulting on changing the abortion regulations, an organisation called Abogados Cristianos (Christian Lawyers) went to the supreme court last April asking it to exclude abortion care from the list of essential services.
They claimed the services remaining open would be “contrary to all health regulations” and “not urgent”. They lost, but the legal representative of the Spanish abortion clinics association (Acai), José Antonio Bosch, said the group had sued 28 abortion clinics all over Spain since 2015.
According to Acai’s vice-president, Eva Rodríguez, these “never-ending lawsuits” take a toll on the association and its staff. “We are not rich, and hiring lawyers or procurators is a costly affair,” said Rodríguez. “It’s exhausting, to always be vigilant. We don’t always win these cases.”
The UK government has not been spared such pressure. Christian Concern labels itself as “one of the most prominent evangelical organisations in the UK”, with just over 40,000 Facebook followers. It has a sister organisation called the Christian Legal Centre that supports its legal cases.
A few days after the UK approved telemed abortion, Christian Concern pursued a legal action against the Department of Health and Social Care, seeking a judicial review of what they called the government’s “incredible double U-turn on DIY abortions”.
According to the group, the advent of telemedicine abortion breaches the 1967 Abortion Act, which was to prevent “backstreet” abortions. The group have since claimed that abortion pills prescribed via telemed had killed women, based on a leaked email sent to an NHS mailing list on 21 May. That email came from a senior chief midwife who had written of the “escalating risks” of the “pills in the post-service”, which included “two maternal deaths”.
The email was cited as evidence in the court hearing for Christian Concern’s legal challenge by a key witness, Kevin Duffy, a former staff member at Marie Stopes International who now supports Christian Concern’s work. The claim was relayed in various outlets, not only in the UK but also in the US, with Fox News reporting: “UK women die from ‘DIY’ home abortions.”
“Yes, there have been two cases of women dying after abortion,” said Dr Suzanne Tyler, the executive director of the Royal College of Midwives. “However, both occurred before pills in the post was implemented and therefore have nothing to do with the new arrangements.”
According to Tyler, one is suspected of being a case of sepsis that was not identified by a doctor, and the other was entirely unrelated to the abortion. “We have not been contacted by midwives concerned about the impact of pills in the post,” Tyler said. The senior midwife in question did not respond to comment from the Guardian, despite numerous attempts to speak to them.
Despite losing the high court bid in May, Christian Concern took its case to the court of appeal, which dismissed it in September. But that has not deterred the group from battling on. It is now taking its case to the supreme court. When asked why telemed abortion was deemed dangerous, Tom Allen from Christian Concern said: “For a start, the government thinks it is dangerous. This is what health minister Lord [James] Bethell said when the service was proposed on the eve of lockdown in March.” He also cited a report in the Sun newspaper on a murder investigation related to the service, and an “undercover investigation” carried out by a consultancy firm run by Duffy.
Underground networks
The inevitable result is that where abortion has been heavily restricted, women have been forced by their circumstances to look to the black market. There are organisations, such as Women on Web (WoW) and Women Help Women, who appear motivated by the best of intentions to get pills to desperate women, using meticulously researched strategies to avoid seizure by customs officials – a problem encountered mainly in Italy and Poland. Last June the Spanish government blocked access to WoW’s website without warning. WoW is now suing the Spanish state, accusing it of failing to comply with its obligations to provide accurate information on sexual and reproductive rights.
But beyond these networks aiding women caught in the worst of situations,others are scamming and offering only further pain and misery.
So-called “pro-life” groups are also increasingly working together. A Christian fundamentalist network called Agenda Europe that formed in the early 2010s as a lobbying group working on behalf of an alliance of conservative organisations has led an offensive against sexual reproductive health and rights efforts in national parliaments. Gender equality, or as they call it “gender ideology”, has become the central, unifying target for this network. Christian Concern and Abogados Cristianos are involved. A document called Restoring the Natural Order sets out the guiding principles: to reverse the “achievements of the cultural revolution” of the 1960s in Europe.
For Dr Dhammika Perera, global medical director at MSI, Europe is at a crossroads – and which way the continent goes will depend on leadership.
“I use the word leadership because it’s not always just the politicians, it’s the politicians, the religious leaders, the community leaders,” Perera said. “We should not say abortion access was restricted due to the pandemic because I don’t think the pandemic is the problem. I think it’s leaders who use it as an excuse to further their efforts to limit abortion.”
Perera said the story of the pandemic was that that it had exacerbated gaps in access to abortion services across Europe. There was a clear danger that this trend would continue.
The practice of telemedicine abortions has only been taken up during the pandemic by five countries – England, Wales, Scotland, France and Ireland – in addition to Denmark and the Stockholm region of Sweden where it was already in use.
In Northern Ireland, abortion provision, whether in hospitals or at home, remains a live issue, with women still battling to secure a safe and accessible service despite legalisation in 2019. Even under the liberalised rules brought in during the pandemic, a first pill for medical abortions still needs to be taken at a clinic.
Demonstrators march through the streets of Belfast ahead of a meeting of the Stormont Assembly on abortion rights. Photograph: Charles McQuillan/Getty Images
Indeed, even among Europe’s abortion providers, abortion via telemedicine remains a subject of debate.
In the Netherlands – often considered to be one of the most liberal countries on abortion rights – a judge rejected a court application in April last year to force the health ministry to make abortion pills available remotely. The ruling means women are still bound by law to visit a clinic before they can be given the medication.
Yvonne Bogaarts, of Rutgers, a Dutch NGO focused on sexual and reproductive health, said the vast majority of abortions in the Netherlands were carried out surgically. Medication-induced terminations make up only 20% to 25%. “We are not sure [telemed abortion] is necessary for our country,” Bogaarts said.
Celia Herrero Medina, of Acai in Spain, echoed that sentiment: “It is better for women, and they tell us continuously, to undergo a medical abortion with the support of a specialised team who can answer all their questions 24 hours a day, rather than they do it alone and be helpless in case they have questions or complications.”
‘How thankful I am to feel safe’
Nevertheless, Perera argues that the recent extension of home abortions by some countries has offered hope that the move towards a closing down of abortion rights can be reversed. “Even among all the misinformation spread, I think that more European countries will realise telemedicine’s benefits for women,” he said.
Kay agrees: “The most traumatic part of the entire process was reading the horror stories online, I imagine from anti-abortionists,” she recalled of her experience last year. “Last night I snuggled up with my daughter after an exhausting day at work and read Peace at Last and thought how thankful I am for this peaceful moment, feeling safe and not afraid for my health or future.”
But since March 2020, indie clinics have reported enormous financial hardships and an urgent need for financial support in order to continue providing care throughout the COVID-19 pandemic. In response, the Women’s Reproductive Rights Assistance Project (WRRAP)—the largest national independent abortion fund in the U.S.—has launched a new initiative to support these clinics and their millions of abortion-seeking patients.
Established to provide supplemental emergency funding for people accessing abortion from indies in all 50 states, the KIIRA Fund is named in honor of WRAPP’s former board member Kiira Jepson, who passed away unexpectedly in 2019.
“Kiira was a die-hard advocate for reproductive justice and rights,” Sylvia Ghazarian, executive director of WRRAP, told Ms. “One of the things she was always about was how we need to continue to support independent clinics.”
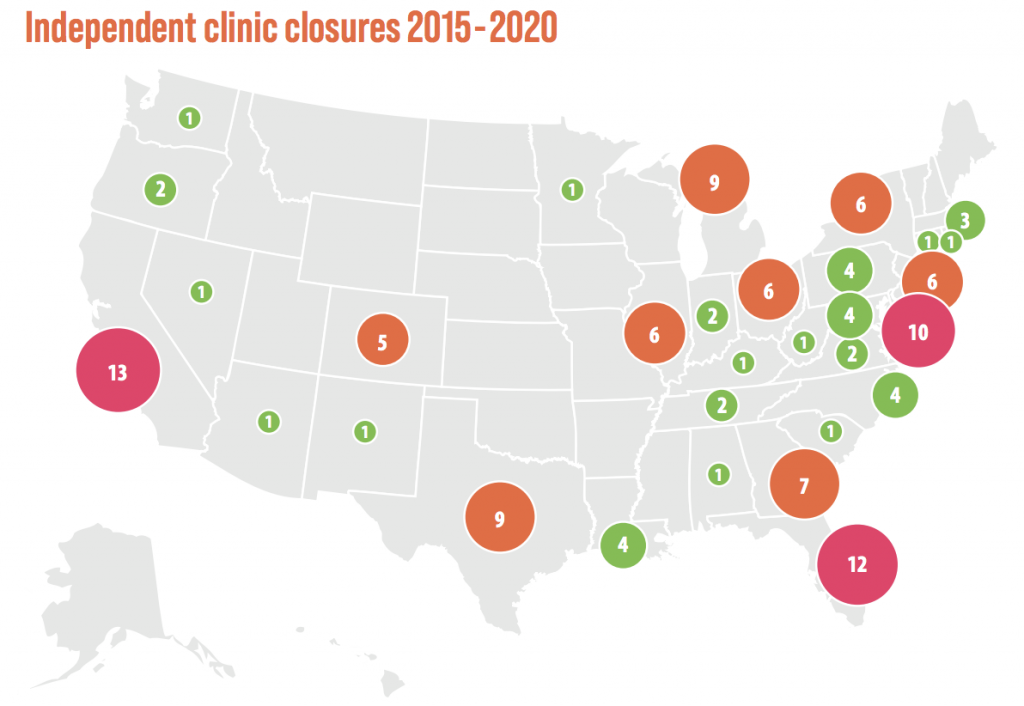
Since March 2020, independent abortion clinics have been shutting down at alarming rates due to the effects of the COVID-19 pandemic. (Robin Marty / Flickr)
Independent clinics have decreased 32 percent in the past decade—from 510 clinics in 2012 down to only 344 as of November 2020. According to the Abortion Care Network, many abortion-seekers don’t have access to a Planned Parenthood or their primary physician for abortion care, so they rely on community clinics. Without indies, millions will lose access to essential health care.
“Independent clinics … don’t have the fundraising coverage that national organizations have,” Ghazarian said.
When Abortion Care Network started tracking clinic closures in 2012, they had identified 510 independent abortion clinics open in the U.S. As of November 2020, ACN identified 337 open independent clinics. (Abortion Care Network)
“What makes WRRAP unique is that we support our sister abortion funds in each state and each county. We are able to support and fund in each of the 50 states,” said Ghazarian.
A majority of WRAPP’s funding goes to low-income women and women of color, according to Ghazarian, and the financial impacts of the pandemic have only exacerbated this need: “Obviously, the biggest portion of our funding is women of color and those who are on or below the poverty line. Being able to navigate COVID plus what they’re going through is just … unreal, right now.”
When asked about Kiira’s legacy and the impact she had on the organization, Ghazarian said:
“She was a sweet, inspiring, beautiful, intelligent beam of light. I came on board with WRRAP three years ago, and she was so generous with training and her time with me and getting to know me. We connected on a personal level, just her being a great person for the community and understanding the fundamental needs of people. It was a great honor to get to know her. She had such an impact on the organization.”
In honor of the late Kiira Jepson’s upcoming birthday on April 25, WRRAP aims to raise $30,000 throughout the month of April.
To donate to the Kiira Fund or to WRRAP, head here. WRRAP is giving bracelets for any gifts or donations over $50—so that, according to Ghazarian, “individuals can show they are supporting someone at an independent clinic and wear it with pride.”
Last month, Women’s History Month came and went with constant reminders that gender-based violence remains all too common: March started in South London with the alleged murder of 33-year-old marketing executive Sarah Everard by a police officer, followed by a massacre in Atlanta that saw six Asian women shot and killed by a white man who was, in his mind, exacting punishment on them for being a sexual “temptation” to him. The month ended with the exposure of Florida Rep. Matt Gaetz’s alleged sexual misconduct with a teenage girl and involvement in sex trafficking.
April marks Sexual Assault Awareness Month, continuing the conversation about gender violence along with the recent uptick in state abortion bans nationwide—the two are deeply, inextricably entwined. With total abortion bans passing in Arkansas, Texas, South Carolina, and other states this legislative session, as well as so-called, “race-based” abortion bans and medication abortion restrictions in North Carolina and Ohio, states have recently escalated their war on pregnant people, with a decisively anti-abortion-friendly bench on the Supreme Court.
These political attacks and acts of state-sanctioned reproductive coercion extend from the same well of misogyny as recent, alarming incidents of gender-based violence, and carry many of the same long-term consequences. Similarly, forced sterilizations allegedly carried out by ICE on immigrant women at the border speak to the disproportionate targets of state reproductive coercion—migrant women and women of color, who are also more likely to experience gender-based violence.
We rarely see the violent connections drawn between abortion bans and sexual assaults, between police violence targeting women of color and anti-abortion politicians equating health care like abortion to murder—but all are rooted in a greater culture of gender violence. Abortion clinics, including providers and patients, are frequently the subjects of menacing acts ranging from sidewalk harassment to arson and shootings, and the reason is simple: When politicians equate abortion with murder, they incite retaliatory violence against those purportedly responsible.
When politicians equate abortion with murder, they incite retaliatory violence against those purportedly responsible.
Following the embattled end of the presidency of the so-called “most pro-life president ever,” divisions among the Republican Party have been reliably bridged by their unwavering unity against women and pregnant people. It’s only April, and 2021 is on track to becoming one of the most dangerous years for state abortion rights in recent history, as increased political attacks on abortion and reproductive care compound with the ongoing pandemic and economic recession, making access to care costlier, and more difficult than ever with added safety risks.
Anti-abortion legislation also dangerously contributes to normalizing intimate-partner violence through reproductive coercion. When state and federal lawmakers constantly attempt to legislate and control the bodies and reproductive health options of women, girls and pregnant people, this sort of coercion becomes culturally acceptable, and is all too often mirrored and reproduced in relationships.
A 2010 study found 15 percent of women who report experiencing physical violence from a male partner also report birth-control sabotage, or their partner tampering with their birth-control pills to force them to become pregnant. Birth-control sabotage seems to disproportionately impact young women and girls—according to the American College of Obstetricians and Gynecologists, a quarter of adolescent girls reported their abusive male partners had attempted to impregnate them without their consent by interfering with their contraception. Sixty-six percent of adolescent mothers on public assistance who reported experiencing domestic violence also reported experiencing birth-control sabotage by their partner. Despite the prevalence of reproductive coercion in relationships, it’s often vastly underreported as many victims aren’t aware that such acts constitute abuse.
Victims of sexual violence and people who experience pregnancy loss or self-induce their abortions also share a concerning commonality: criminalization. Those who experience sexual violence are significantly more likely to face charges or be incarcerated than perpetrators—90 percent of incarcerated women, who are disproportionately women of color, are survivors of sexual assault, while it’s estimated just five out of 1,000 rapists will ever be imprisoned.
In a similar vein, feticide laws and stigma around abortion and miscarriage are often weaponized against people who lose their pregnancies or self-manage their abortions with medication, to charge them with feticide, child endangerment, abuse of a corpse, and other charges. Notably, in 2019, a Black woman named Marshae Jones faced charges for manslaughter in Alabama after being shot in the stomach and experiencing a miscarriage. Police pressed charges against Jones as they alleged she had started the fight that led to her miscarriage. Stories like this have frequently unfolded across the country in recent years: Purvi Patel, an Asian-American woman in Indiana, faced jail time for allegedly taking medication abortion and having a stillbirth in 2013.
When it comes to the criminalization of survivors and those who are victimized by state policies on pregnancy and reproduction, the message is clear: The rights to safety and bodily autonomy still don’t belong to all of us, and women and pregnant people remain subhuman under the law.
One Oklahoma lawmaker inadvertently said the quiet part out loud in 2017, as he defended a law to require consent of the father of the fetus for someone to have an abortion: “I understand that they feel like that is their body,” he said of pregnant women. “I feel like it’s separate—what I call them is, you’re a ‘host.’” Republicans Todd Akin and Steve King have both drawn bipartisan criticism for arguing against rape exceptions to abortion bans, but many of these criticisms have ignored that with or without so-called rape exceptions—which send the false message that rape is easy to report and “prove” to police or medical professionals—all abortion bans are a violation of consent. Consent to sex has never meant consent to pregnancy, and forced pregnancy and birth often amount to a deeply traumatic violation of someone’s body and life.
Language, legislation, and political attacks by anti-abortion politicians have always made it devastatingly clear that the humanization of fetuses consequently dehumanizes pregnant people. This reality is inseparable from a greater culture of gender violence that systematically victimizes, blames, and even kills women and girls. Reproductive coercion is gender violence—and all gender violence is rooted in denying women and non-cisgender men humanity and autonomy.
On April 12, FDA Acting Commissioner Janet Woodcock, MD, said the agency would temporarily stop enforcing the requirement under Risk Evaluation and Mitigation Strategy (REMS) guidelines that mifepristone, the first drug in a two-drug regimen taken for medication abortion, be dispensed by a doctor. For the remainder of the COVID-19 pandemic people can receive it by mail.
Colleen McNicholas, DO, obgyn and Chief Medical Officer at the Planned Parenthood of the St. Louis Region and Southwest Missouri, explained to POPSUGAR that whether you had to actually take the first drug in the health centre or doctor’s office, or you could instead go pick it up and then bring it home with you, completely depended on state law. The American College of Obstetricians and Gynecologists (ACOG), which was among one of the groups who sued to suspend the distribution requirement, wrote in a statement that mifepristone has proven to be a “safe, effective medication,” and that in-person dispensing during the pandemic was dangerous and burdensome, especially for those hit hardest by the pandemic including low-income communities and communities of colour.
The Guttmacher Institute estimates that in 2017, 39 percent of abortions were medication abortions, and among abortions that happened within a 10-week gestation window, medication abortions accounted for 60 percent that year. Ahead, find out more about medication abortions.
How Do Abortion Pills Work?
The FDA first approved mifepristone, known as Mifeprex, in 2000, and it is ordered, prescribed, and dispensed by a qualified healthcare provider up to 70 days — or up to 77 days in some cases — of pregnancy (the FDA decision from this week makes it easier for mifepristone to be distributed by mail). Then, 24 to 48 hours after taking Mifeprex, a different pill, misoprostol, is taken in the location of your choice, meaning it can be administered at home.
Dr. McNicholas said mifepristone stops a pregnancy from progressing because it blocks progesterone, one of the hormones that holds the pregnancy to the uterus. Misoprostol then causes the uterus to contract and results in cramping and bleeding that expels pregnancy tissue, which usually starts in one to four hours. According to Planned Parenthood’s national website, nausea, mild fever, tiredness, heavy bleeding with large clots, and dizziness are also side effects from taking misoprostol. Nausea and slight bleeding may begin after taking mifepristone, though it’s not common.
Expelling the pregnancy tissue can usually last five hours or longer, and the cramping may persist for a few days. Planned Parenthood noted that if you don’t have any bleeding within 24 hours of taking misoprostol, you should call your doctor. You’ll have a followup appointment a week or two after the medication abortion, which Melissa Grant, COO of abortion and reproductive health service provider Carafem, told POPSUGAR can happen virtually (after checking in about symptoms, providers may later ask you to take a home pregnancy test to confirm a negative test result).
How you qualify for a medication abortion pill will depends on where you live, but in terms of gestation, Dr. McNicholas explained, the FDA approved the medication through 70 days of gestation, and the medical community has since developed and supported use up to 77 days.
How Effective Is the Abortion Pill?
According to Planned Parenthood, if you are eight weeks pregnant or less, a medication abortion works about 94 to 98 percent of the time. For people who are between 10 and 11 weeks pregnant, it’s about 87 percent effective. Though rare, if the abortion doesn’t work and you’re still pregnant, you may need additional medication or to go for an in-clinic procedure. Complications from medication abortion are also rare but could include pregnancy tissue left in the uterus, infection, allergic reaction, blood clots in your uterus, and too much bleeding. Call your doctor if you feel sick more than 24 hours after taking misoprostol.
Both Grant and Dr. McNicholas wanted to stress that mifepristone and misoprostol used for medication abortion are not only effective but safe. “It’s really important that regardless as to whether we’re in a pandemic or not, that people, particularly in a country as advanced as the United States, should be able to have access to the health care that they want, that they are medically eligible for, and that they deserve,” Grant said. “The additional barriers do nothing to make it safer and, if anything, actually delay appointments, increase costs, and create more stress and strife for the people in the situation.”
Where Can You Get Abortion Pills?
Typically, you get these pills from a doctor’s office or clinic such as Planned Parenthood or Carafem. Grant suggests using the National Abortion Federation as a resource where you can find a list of accredited providers from across the country. Some doctors will give mifepristone to you in their office and then write a prescription for misoprostol to pick up at a pharmacy separately, or they might have misoprostol at their disposal already and send you home with it (now it will be easier to get both sent to you via mail or through a mail-order pharmacy). The cost varies and also depends on many factors like the facility you go to, state law, other tests you may need to get before or after your medication abortion, and insurance coverage.
The FDA’s decision opens up the opportunity for telemedicine visits, such as the service Abortion on Demand. And as of Tuesday, the Planned Parenthood of the St. Louis Region and Southwest Missouri offered telemedicine for medication abortions, what Dr. McNicholas called “direct-to-patient” visits.
You can also check out the TelAbortion Study, a clinical study sponsored by reproductive health nonprofit Gynuity Health Projects that uses telemedicine for medication abortions and sends these drugs through the mail. The project is currently available through certain Planned Parenthood locations, Carafem, and other partners for people living in Colorado, Georgia, Hawaii, Illinois, Iowa, Maine, Washington DC, Maryland, Massachusetts, Minnesota, Montana, Nevada, New Jersey, New Mexico, New York, Oregon, Virginia, and Washington. The TelAbortion Study is ongoing, and data collected about the effectiveness of telemedicine medication abortions versus procedural and medication abortions done in-person will continue likely until the restrictions on sending mifepristone through the mail are lifted indefinitely, not just for the duration of the pandemic.
Carafem has participated in the study since 2017. “We did this primarily because we serve a large number of rural clients, particularly in the south and in the midwest, who are travelling great distances to receive medication abortions,” Grant said. Additionally, Carafem just launched a virtual health care assistant, fittingly named Cara, to act as a 24-hour support service.
A Win, but Not a Complete Victory For Medication Abortions
“When we have big federal wins like this, where the FDA is approving access, that access gain isn’t appreciated for everybody equally.”
“The rules and regulations that guide abortion care unfortunately oftentimes sit squarely in the political realm and not just in the medical and scientific realm,” Dr. McNicholas said. “When we have big federal wins like this, where the FDA is approving access, that access gain isn’t appreciated for everybody equally.”
Grant noted that abortion is not an uncommon experience (the abortion rate in 2014 was one in four by age 45), adding that untended pregnancies are often complicated by financial instability and inadequate access to healthcare. “It’s important that people have safe options that are respectful of their own personal needs, their own personal belief systems, if they decide that they want to have an abortion,” she said. “Whether you prefer to have your abortion at home with a pill, in the clinic with medication, in the clinic with a procedure and maybe additional pain killer, these are all legal, safe options the patient themselves should be able to choose.”
Image Source: POPSUGAR Photography / Matthew Kelly
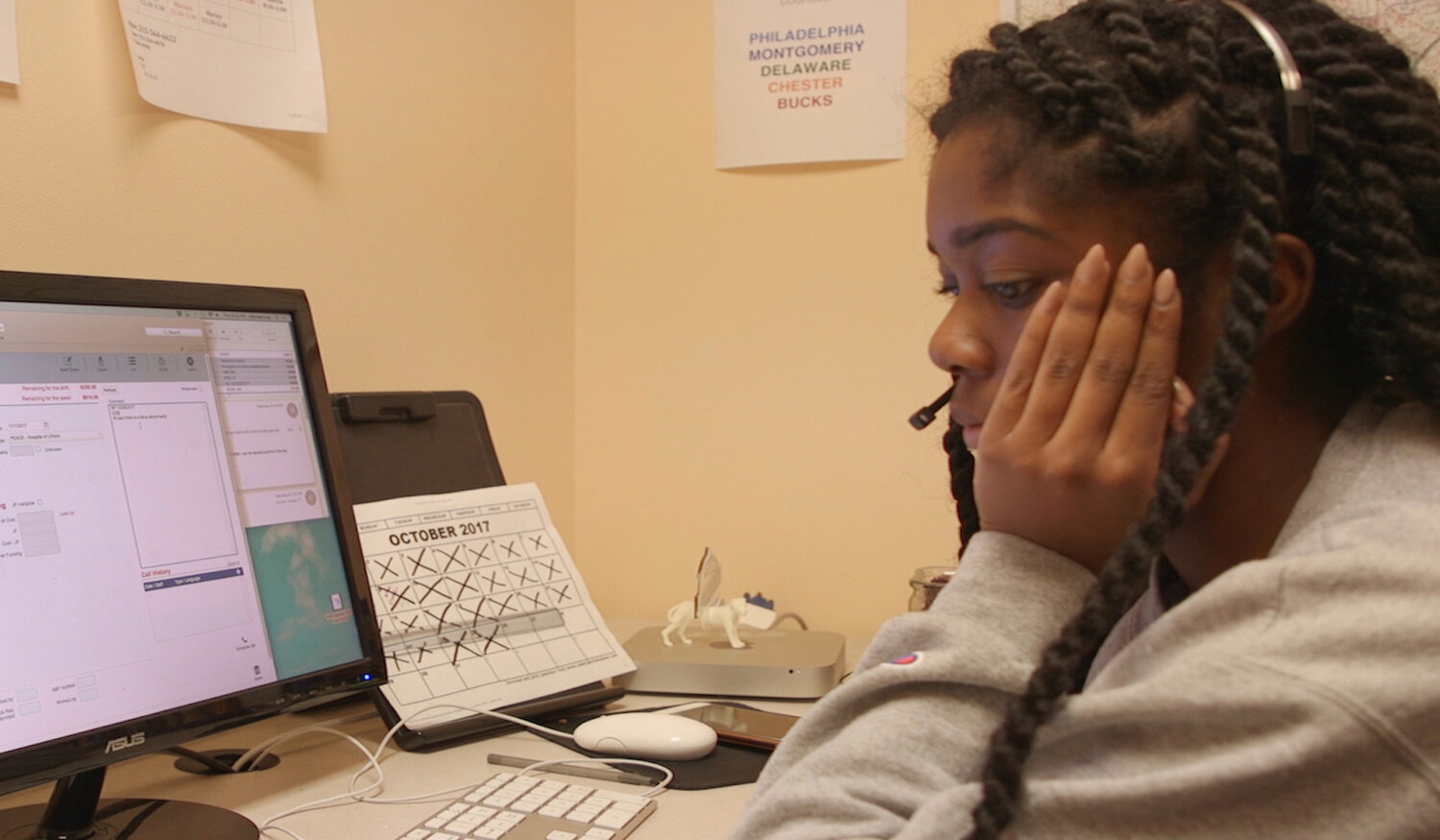
“Abortion Helpline, This is Lisa” is a national rallying cry: It’s time for the Hyde Amendment to end. (Abortion Helpline, This is Lisa)
Oscar-shortlisted documentary short “Abortion Helpline, This is Lisa” is 13 gut-wrenching minutes of the impacts of the Hyde Amendment, showcasing the devastating reality of the lack of abortion access in the U.S.
When the difference between feeding your kids, forgoing your life-saving medication, or losing everything in your life is $275, what do you do when there’s no one left to call? This is the question viewers are left with when watching “Abortion Helpline, This is Lisa,” a short documentary film offering a glimpse into the lives of five callers to an abortion fund hotline in Philadelphia—each left with an unplanned pregnancy, no options, and everything to lose.
At the Women’s Medical Fund, the counselors depicted in the film (all referred to as Lisa) are often the last call before there’s no one left for thousands of people every year. One caller in the film—who needs only $275 more for her abortion—has already survived one life-threatening pregnancy, has just lost her job, and barely has enough left for groceries.
“All my savings that I had are going towards my insulin and making sure my kid is set,” she tells Lisa, “I have $100 and have enough to cover my rent for this coming month.” The film glaringly shows us the counselor’s computer screen: There’s only $19 left in funds for the current shift. They will need to call again tomorrow and hope there will be more.
Hope is not going to be enough, but it is all viewers are left with—we never learn how this caller’s situation turns out. The outlook is grim: People who are denied wanted abortions are four times more likely to live below the federal poverty line, and three times more likely to be unemployed than people who receive an abortion, leaving them with chronic economic insecurity. Additionally, those who are denied abortions are more likely to experience complications during birth, raise the child on their own, and remain in an abusive partnership.
Directed by Janet Goldwater, Barbara Attie and Mike Attie, “Abortion Helpline, This is Lisa” is 13 gut-wrenching minutes of the impacts of the Hyde Amendment, showcasing the devastating reality of the lack of abortion access in the United States. The film has been sweeping through global film festivals, and was recently named to the 93rd Academy Awards shortlist.
Remote care amid COVID-19 illustrates abortion rights are resilient even in the face of a hostile Supreme Court or state laws designed to gut them.
Near-total bans on abortion became law recently in Arkansas and South Carolina, suggesting a dire future for abortion rights if the Supreme Court overturns Roe v. Wade — a possibility that seems more likely than ever before. But the road ahead will not be shaped by anti-abortion legislators or Supreme Court justices alone. A different path to abortion access has emerged.
Over the past year, new virtual clinics have begun delivering medication abortion entirely remotely. Last July, a federal court suspended a Food and Drug Administration rule that requires patients to obtain the first drug in a medication abortion at a health care facility during the pandemic.That drug, mifepristone, is the only one of 20,000 FDA-regulated medications that requires in-person dispensation but can be taken at home.
The ruling created an opening for virtual clinics like Choix, Hey Jane and Just the Pill to offer “no touch” services for people less than 10 weeks pregnant. Patients complete a medical history form online, consult with a clinician over video or telephone, and if eligible, receive two medications from a mail-order pharmacy.
An ongoing study one of us is leading at the University of California, San Francisco (UCSF) demonstrates that the care offered by virtual clinics is safe and effective. The California-based company, Choix, served approximately 140 patients over two months. Patients were overwhelmingly satisfied with the service. It allowed them to have an abortion with privacy and without having to take time off work, find child care or travel long distances. One grateful patient called it a godsend to be able to go through the process while safe at home.
In front of the White House on March 09, 2021, in Washington, D.C. SHANNON FINNEY/GETTY IMAGES FOR THE CENTER FOR HEALTH AND GENDER EQUITY
The same results bear out for Hey Jane, which provides services in Washington and New York and saw demand double week after week in the first month of operation. “I especially loved the fact that the medication came to my house via mail,” said Nicollette Roe, a Hey Jane patient. “I made a plan with my partner about doing it at night, after our daughters were asleep. I had no stress around how to do everything because Hey Jane made it so that the doctor was moments … away via the app or by calling.”
At the moment, these virtual clinics cannot use mail-order pharmacies to deliver medications to their patients. That’s because in January, the Supreme Court reinstated the FDA rule while litigation is ongoing.But virtual clinics illustrate the resilience of abortion care even in the face of a hostile Supreme Court or state laws designed to gut abortion rights.
After the Supreme Court’s order, networks of advocates and providers figured out how to provide abortion outside of brick-and-mortar operations, regardless of a patient’s residence. Start-ups have found innovative ways to deliver medication abortion to patients, like Just the Pill’s pop-up mobile sites. And nonprofit organizations such as Aid Access and Plan C have helped people receive medications by mail regardless of the state in which they live.
Stop unscientific abortion regulation
Remote care is all the more important given the number of states that make gaining access to abortion as difficult as possible and the prospect that the Supreme Court will abandon the core holding of Roe v. Wade. But even if Roe remains on the books, Americans in roughly half of the country live in states without meaningful access to abortion care. The expansion of medication abortion will help navigate these “abortion deserts,” or regions where patients must travel over 100 miles to reach a clinic. Virtual care can overcome the barrier of distance (and its related costs) by reaching patients at their homes and across state borders.
This month, in deciding whether to defend restrictions on medication abortion, the FDA will consider the public health evidence that supports extending virtual services. The UCSF study and others like it provide the proof that remote care is safe and effective — without the financial, social, logistical and interpersonal constraints of clinic-based services. Over the long run, the FDA should allow studies on telehealth for abortion to proceed, enabling a formal review of the safety of direct-to-patient dispensing without the interference of politics. More immediately, the FDA should suspend the unnecessary and scientifically unsupported regulation of medication abortion.
Telehealth may well be the future of more affordable and more accessible abortion care in the first 10 weeks of pregnancy. The Biden administration must act now to help realize that future.
HONOLULU (AP) — Gov. David Ige on Monday signed legislation that would make Hawaii the latest state to allow some nurses to perform abortions.
Hawaii law previously said only physicians could perform early, in-clinic abortions. But because of a doctor shortage, several smaller islands lack abortion providers which forces residents of those islands to fly to Honolulu if they need the procedure.
“This act will enable people who desperately need reproductive health care services to receive health care from very high quality health care providers, including advanced practice registered nurses, where they need it, when they need it, and … in their own communities,” Laura Reichardt, the director of the Hawaii State Center for Nursing, said a bill signing ceremony.
The new law, which took effect when the governor signed it, allows advanced practice registered nurses to prescribe medication to end a pregnancy and to perform aspiration abortion, a type of minor surgery during which a vacuum is used to empty a woman’s uterus. The nurses will be able to do both during the first trimester of a pregnancy. The aspiration abortion may be performed in a hospital, clinic or nurse’s office.
Advanced practice registered nurses are nurses who have obtained at least a master’s degree and are trained and certified to diagnose and manage patient problems and prescribe medications.
Several states already allow this category of nurses to perform medication or aspiration abortions, including California, Colorado, Maine, Massachusetts, Montana, New Hampshire, Virginia, Vermont and West Virginia.
Hawaii has a long track record of favoring abortion rights. In 1970, it became the first state in the nation to allow abortion at a woman’s request.
But the state’s doctor shortage means that the islands of Kauai, Molokai and Lanai have lately lacked local abortion care providers. On the Big Island, abortion has only been available in Hilo but not on the west side. On Maui, a provider has had to fly in from another island twice a month.
Early in the coronavirus pandemic, doctors weren’t able to fly to Maui and abortion care was unavailable on the island for several months, said Dr. Reni Soon, the chairperson of the Hawaii Section of the American College of Obstetricians and Gynecologists.
The legislation Ige signed said studies have found abortions provided by a qualified licensed health care provider other than physicians were just as safe as those provided by doctors. Advocates say advanced practice registered nurses already provide procedures that are similar to or more complicated than abortions, such as inserting an IUD and conducting an endometrial biopsy.
Most testimony to the Legislature supported the new law. Those in opposition included groups that oppose abortion more broadly and those concerned that advanced practice registered nurses wouldn’t have the same training as doctors.
Arkansas, Indiana, Louisiana, Ohio, and Texas all have enacted laws regulating the disposition of fetal tissue (though all but Indiana’s have been blocked by the courts). Getty Images
If we’re so afraid of death—and we are—then equating fetal burial legislation with abortion will only impede access.
Americans are afraid of death. Like, really afraid of it.
It’s this reticence to embrace the inevitable, with healthy open discussions and accessible care, that makes the funeral industrial complex a thriving, moneymaking machine. The U.S. funeral industry is currently estimated at about $16 billion market size, with the median U.S. funeral costing around $7,640. It’s an industry fraught with cost barriers, old-school and outdated practices, and an aversion to progress.
So what happens when you cross that with the anti-abortion movement? Well, as you might imagine, it’s not great.
You’ve probably heard of fetal burial laws, which require the disposition of fetal tissue in a manner similar to that of well … a dead person. Most recently, an Ohio judge temporarily blocked the enforcement of a fetal burial law, which requires the burial or cremation of fetal remains. It was signed into law by Republican Gov. Mike DeWine last December; the judge’s decision earlier this month was handed down a day before the law was set to go into effect.
But the Ohio fetal burial law is far from unique. Arkansas, Indiana, Louisiana, and Texas all have enacted laws regulating the disposition of fetal tissue (though all but Indiana’s have been blocked by the courts), and lawmakers in numerous other states have introduced similar legislation.
Fetal burial laws are harmful for a number of reasons. For starters, they’re an abortion restriction, which means they’re de facto unecessary and dangerous. But you might be asking: If they’re legislating the disposal of fetal remains, doesn’t that mean the abortion has already happened? So how is it a restriction?By invoking images of death through the requirement of burying or cremating fetal tissue, lawmakers are forcing patients to confront their abortion decision as a death.
And honestly, that’s a solid question. Fetal burial laws are insidious the same way laws that require abortion providers to have admitting privileges at local hospitals are insidious: They force providers into agreements with outside organizations that may not be amenable, and in many circumstances are openly hostile, to what abortion providers do. What ends up happening is that a clinic can’t find a hospital—or in this case, a funeral home—to help it comply with these laws, forcing it to close.
But fetal burial laws invoke an even more nuanced obstruction to care by playing into the country’s largely death-phobic nature. Death-phobia is more than just the fear of death and dying: It’s a culture of shame and stigma surrounding death and end of life that breeds anxiety and misunderstanding.
Progressive death-care workers, like those at the Order of the Good Death (where I work as a social media contributor), are pioneering a movement, deemed death positive, to combat the toxic culture around death in the United States, and instead encourage open communication about death and a shift toward understanding that shrouding death in silence does more harm than good.
By invoking images of death through the requirement of burying or cremating fetal tissue, lawmakers are forcing patients to confront their abortion decision as a death. But many don’t see abortion as a death or loss of life at all. And while we know that some people do grieve their abortions as they would a pregnancy loss, we also know that for many people abortion brings on feelings of relief and everything in between.
This forced association could cause patients to forgo or second guess an abortion because of the guilt or ill feelings it evokes, just like laws requiring fetal ultrasounds. These laws are, by design, a cruelty; subjecting pregnant people who choose abortion to emotional torment in the hopes that it will delay or exhaust them into changing their mind. And if they fail to change their mind, laws like those mandating fetal burial make sure that no matter how you feel about your abortion, it’s going to be a heavy and traumatic experience.
Invoking death-phobia to restrict abortion is not unique to fetal burial laws—other laws like those mandating perinatal hospice, which would require a person to carry an unviable pregnancy to term instead of having an abortion, also play to our fears and inability to talk about death openly.
Lawmakers who support fetal burial laws are counting on this country’s death-phobia. They need constituents to hear words like “cremation” or “remains” and recoil. If we’re so afraid of death—and we are—then equating it with abortion will only impede access.
FILE – This Sept. 22, 2010 file photo shows bottles of the abortion-inducing drug RU-486 at a clinic in Des Moines, Iowa. On Tuesday, April 13, 2021, the acting head of the Food and Drug Administration said women seeking an abortion pill will not be required to visit a doctor’s office or clinic during the COVID-19 pandemic, in the latest reversal in ongoing legal battles over use of the medication. (AP Photo/Charlie Neibergall)
WASHINGTON (AP) — Women seeking an abortion pill will not be required to visit a doctor’s office or clinic during the COVID-19 pandemic, U.S. health officials said Tuesday in the latest reversal in an ongoing legal battle over the medication.
The Food and Drug Administration announced the policy change a day earlier in a letter to the American College of Obstetricians and Gynecologists, one of several medical groups that has sued over the restriction put in place under the Trump administration.
The FDA’s acting head, Dr. Janet Woodcock, said an agency review of recent studies “do not appear to show increases in serious safety concerns,” when women take the pill without first visiting a health facility and discussing the drug’s potential risks, including internal bleeding.
The change clears the way for women to get a prescription for the pill — mifepristone — via telemedicine and receive it through the mail. However, abortion opponents are pushing legislation in several Republican-led states that would head off easier access.
Medication abortion has been available in the United States since 2000, when the FDA approved the use of mifepristone. Taken with a hormone blocker called misoprostol, it constitutes the so-called abortion pill. About 40% of all abortions in the U.S. are now done through medication — rather than surgery — and that option has become more pivotal during the COVID-19 pandemic.
Last year, the FDA waived in-person requirements for virtually all medications, including tightly controlled drugs such as methadone. But the FDA and its parent health agency argued the rules were necessary to ensure the pills were used safely. The rule requires patients to pick up the single tablet of mifepristone at a hospital, clinic or medical office and sign a form that includes information about the medication’s potential risks.
The obstetricians and gynecologists group sued to overturn the rule, setting off a series of conflicting court decisions. Most recently, in January, the Supreme Court sided with the Trump administration to reinstate the longstanding rule on getting the drug in person.
The obstetricians group said in a statement Tuesday the FDA’s about-face on the requirement shows “it is arbitrary and does nothing to bolster the safety of an already-safe medicine.”
The move was also hailed by congressional Democrats, some of whom had called on FDA to reverse its policy in a February letter.
But abortion opponents said the move would jeopardize women’s health.
“With this action, the Biden administration has made it clear that they will prioritize abortion over women’s safety,” said Jeanne Mancini, president of the anti-abortion group March for Life. “Chemical abortions should have more medical oversight, not less.”
The FDA policy only applies during the COVID-19 health emergency. The obstetricians and gynecologists group and several other medical organizations are pushing to make medication abortion permanently available via online prescribing and mail-order pharmacies.