The language of Thursday’s order suggests the Supreme Court was simply unwilling to make any decision in an abortion case three weeks after Justice Ruth Bader Ginsburg died and just days before Judge Amy Coney Barrett confirmation hearings. J. Scott Applewhite/AP
The U.S. Supreme Court has refused, for now, to reimpose FDA regulations that require women seeking medication abortion to pick up the prescribed pills in person at a clinic instead of by mail.
The court’s decision came Thursday night on a 6-to-2 vote that rejected an emergency appeal from the Trump administration.
The challenge to the Food and Drug Administration regulation was brought by the American College of Obstetricians and Gynecologists after the the agency relaxed similar regulations for other drugs — including opioids — in order to limit patients’ exposure to COVID-19 during the pandemic. The FDA refused to relax the same rule for those with prescriptions for abortions with pills in the first 10 weeks of pregnancy.
Federal Judge Theodore Chuang in Maryland ruled in favor of ACOG, declaring that requiring such in-person pickups of pills during a pandemic posed “a substantial obstacle to women seeking an abortion.” The Supreme Court has long ruled that such substantial obstacles unconstitutionally interfere with a woman’s right to terminate a pregnancy.
On Thursday night, the Supreme Court turned down the Trump administration’s attempt to block the lower court order. But the decision was more of a punt than a long-lasting decree.Article continues after sponsor message
The high court said it would hold the Trump administration’s request “in abeyance” to permit the district court judge to promptly consider other efforts by the administration to “dissolve, modify, or stay” its previous order if “relevant circumstances have changed.” And the justices said that their decision did not indicate their views on the merits of the case should it come to them again.
The language of the one-paragraph order seemed to suggest that the court was simply unwilling to make any decision in an abortion case three weeks after Justice Ruth Bader Ginsburg died, and just days before the U.S. Senate is scheduled to take up the nomination of Judge Amy Coney Barrett as Ginsburg’s replacement.
“It is a relief that for the next few weeks, the Trump administration cannot force abortion patients to needlessly risk contracting a life-threatening disease as a condition of obtaining care,” said Julia Kaye, lead counsel for ACOG in the case. But, she added, “When President Trump is trying to rush through a third Supreme Court justice with the express goal of overturning Roe v. Wade, the court’s delayed ruling in this case gives little comfort that the right to abortion is secure.”
But Marjorie Dannenfelser, president of the Susan B. Anthony List, which opposes abortion rights, said her group was “disappointed by the lack of a ruling.”
“We thank the Trump administration for fighting for vitally important health and safety protections and are confident we will ultimately prevail,” she said.
Dissenting from Thursday night’s decision were Justices Samuel Alito and Clarence Thomas. Writing for the two, Alito said that “for all practical purposes there is little difference between what the court has done and an express denial” of the Trump administration’s emergency motion to block the lower court order.
Alito went on to blast his colleagues for other actions it has taken during the pandemic in upholding bans on large church gatherings, decisions that he characterized as “unimaginable restraints” on the “free exercise of religion.”
Resolution calls for promoting, protecting and respecting women’s and girls’ full enjoyment of human rights in humanitarian situations
The Center for Reproductive Rights welcomes the United Nations Human Rights Council’s (HRC) adoption by consensus in Geneva today of a resolution titled “Promoting, Protecting and Respecting Women’s and Girls’ Full Enjoyment of Human Rights in Humanitarian Situations.”
The resolution recognizes that humanitarian situations—such as those caused by conflicts and natural disasters—may cause and exacerbate gender discrimination and existing inequalities.
The resolution is the first ever to meaningfully consider women’s and girls’ full enjoyment of human rights in humanitarian situations as a stand-alone issue, and highlights the applicability of human rights for all women and girls, in all contexts.
“Women and girls in humanitarian settings face barriers when seeking justice for the human rights violations they have endured,” said Rebecca Brown, Senior Director for Global Advocacy at the Center for Reproductive Rights. “Rights-based accountability must therefore be prioritized and we commend the core group for their leadership in putting this issue on the agenda of the Human Rights Council.”
Canada, Fiji, Georgia, Sweden, and Uruguay formed the core group behind the resolution.
In 2018, an estimated 34 million women of reproductive age, at least five million of whom were pregnant, were in need of humanitarian health assistance due to conflict, according to a recent report from the Center for Reproductive Rights and LEDAP. The Boko Haram insurgency, for instance, has resulted in hundreds of thousands of internally displaced people living in settlements in Nigeria, where there have been countless stories of abuse with no accountability. Between 2009 and 2016, according to the United Nations Population Fund, over 2.2 million people were internally displaced because of the insurgency, and as many as 7,000 women and girls abducted.
The resolution, which enjoys the support of 47 UN Member States, advances a comprehensive approach to promoting, protecting and respecting women’s and girls’ full enjoyment of human rights in humanitarian situations and highlights the need for accountability, as well the need for the agency and experiences of women and girls in humanitarian situations to be central in humanitarian response.
Resolution Recognizes Increased Barriers Faced by Women and Girls
This is the first resolution that gives a mandate to the Office of the United Nations High Commissioner of Human Rights to report on a comprehensive approach to promoting, protecting and respecting women’s and girls’ full enjoyment of human rights in humanitarian situations.
The resolution:
Acknowledges the interlinkages and complementarity of international human rights and humanitarian law, as well as the applicability of international human rights law in humanitarian situations.
Defines humanitarian situations as situations including humanitarian emergencies, forced displacements, armed conflicts and natural disasters, including sudden-onset natural disasters, and slow-onset events.
Recognizes that humanitarian situations have the potential to exacerbate pre-existing, or create new, patterns and structures of discrimination and inequalities, and further undermine access to health care services and information, housing, water, sanitation, education and employment, and may disrupt protection systems, resulting in a disproportionately negative impact on the enjoyment of human rights by women and girls.
Recognizes that in humanitarian situations women and girls face increased barriers to access to justice and remedies for all human rights violations and abuses they experienced, thus hindering accountability from being ensured.
Emphasizes the importance of women’s and girls’ meaningful participation, empowerment and leadership, including that of survivors and victims, in efforts to prevent, reduce risk of, prepare for, resolve and rebuild from humanitarian emergencies, as well as the need for a comprehensive approach to promoting, protecting and respecting women’s and girls’ full enjoyment of human rights in humanitarian situations.
Requests the United Nations High Commissioner for Human Rights to submit to the Human Rights Council at its 49th session an analytical report on a comprehensive approach to promoting, protecting and respecting women’s and girls’ full enjoyment of human rights in humanitarian situations, including good practices, challenges and lessons learned at the national, regional and international levels, with input from all relevant stakeholders, including Member States of the United Nations, United Nations bodies, agencies, funds and programmes, the treaty bodies, the special procedures of the Council, national human rights institutions, civil society organizations, and women and girls in humanitarian situations.
All women and girls in humanitarian settings urgently need sexual and reproductive health care and services. The provision of sexual and reproductive health information and services is a crucial component of rehabilitation and reparations for victims and survivors and should not be overlooked.
The Center for Reproductive Rights works on ensuring respect for, and protection and fulfillment of, women’s and girls’ sexual and reproductive health and rights in humanitarian situations through various projects in nations including Colombia, Nigeria and Uganda and at the global level at the UN Security Council and the UN Human Rights Council.
Justice Ruth Bader Ginsburg was one of American Civil Liberties Union’s (ACLU) most illustrious alumni. She founded the ACLU’s Women’s Rights Project and in the weekend following her passing, the ACLU renamed its Center of Liberty to the Ruth Bader Ginsburg Center of Liberty.
When Justice Ginsburg embarked on her legal career at the ACLU, there were hundreds of laws on the books that discriminated on the basis of sex. Ironically, these laws were predicated on “protecting women.” For example, women were prohibited from jobs that required them to work at night or to work where she would be required to carry or lift more than 15 pounds.
Before Justice Ginsburg, arguments to get rid of sex discrimination never prevailed in the court. She changed that; she changed history. In her short tenure at the ACLU, Justice Ginsburg played a significant role in 34 Supreme Court cases. She argued six cases before the court herself and prevailed in five of them. In her first oral argument before the Supreme Court, there was not one single question from any of the nine justices. Many observers described the justices as “transfixed.”
Justice Ginsburg was a person ahead of her time — a visionary architect of legal protection for women’s rights and gender equality. She possessed the then-radical belief that laws steeped in gender stereotypes hurt both women and men. Laws derivative of patriarchal notions of what it means to be a man or a woman deprive us all of the freedom to control our own lives. Significantly, she viewed reproductive freedom as a necessary component of true gender equality and dedicated her life’s work to ensuring law was used as a tool to advance equality.
Like many, I thought that between her work ethic, her workout routines and the many health bouts where she came out ahead, Justice Ginsburg would live longer than she did. Her loss comes at a pivotal time for reproductive freedom, in particular, as opponents of reproductive freedom and gender equality work strategically to roll back abortion rights nationally and here in Colorado. If Republicans retain control of the nomination and confirmation process, Justice Ginsburg’s replacement will without doubt wear their hostility to reproductive rights as a badge of honor. The recently named nominee, Judge Amy Coney Barrett, has vowed to overturn Roe v. Wade if confirmed. And a newly configured Supreme Court won’t stop there. Health care, climate protection, voting rights, and immigrant rights all hang in the balance now that Justice Ginsburg is no longer on the bench.
Here in Colorado, we are fighting our own reproductive freedom battle at the ballot: Proposition 115. This measure bans abortion later in pregnancy and denies women the ability to make their own personal medical decisions. The proponents of this initiative are clear — they want to force a woman to continue a pregnancy with no exceptions for health or individual circumstances — even in cases of rape, risks to the woman’s health, or a lethal fetal diagnosis. Prop 115 is a one-size-fits-all mandate that fails to acknowledge that every pregnancy is unique and shows no compassion for Colorado women and families faced with unimaginably complicated circumstances.
Let me be clear: all abortion bans — whether in Alabama or Colorado — are political attacks. They are not about health or medicine. They are about controlling women and taking away decision-making power. This is evidenced by the fact that Proposition 115 is being pushed by many of the same politicians and groups who have tried — and failed — to ban abortion altogether in Colorado every year for the last decade. If Proposition 115 succeeds in Colorado this November, it will embolden the proponents to pursue bans even earlier in pregnancy, with the ultimate goal of restricting all abortion access in Colorado and across the country.
In the landmark 1973 Supreme Court case Frontiero v. Richardson, the then-ACLU attorney and future Justice Ginsburg argued in favor of striking down a law that prevented women in the military from receiving dependent benefits for their husbands. Quoting famed abolitionist and equal rights advocate Sara Grimke, Ginsburg said “I ask no favor for my sex. All I ask of our brethren is that they take their feet off our necks.” Proposition 115 bestows no special right or favor for women, but it certainly advocates controlling women’s choices and constraining their autonomy.
These are the freedoms that Justice Ginsburg worked tirelessly to achieve for the last half-century. Now that she is gone, let us honor her legacy by fighting to protect gender equality and reproductive rights. Vote “NO” on Proposition 115.
Denise Maes is public policy director of the American Civil Liberties Union in Colorado.
Proposition 115 would ban abortions after 22 weeks except when the pregnant person’s life is immediately threatened.
If Proposition 115 were to pass, it could have ripple effects far outside of Colorado. For one thing, people out of state travel there for abortions later in pregnancy. Michael Ciaglo/Getty Images
Amy Lynn learned about a severe neural tube defect during her 20-week ultrasound in 2008. She got an appointment with a perinatologist in Denver the next day and saw a pediatric neurosurgeon the day after that. In her 21st week of pregnancy, she had a dilation and evacuation abortion.
Lynn said she and her husband were “incredibly lucky”: to get the specialist appointments so quickly, to live near those providers, and to have family help pay for the procedure when insurance initially denied it. Even so, her procedure was just a day or two before the abortion cutoff that a November ballot initiative seeks to impose in Colorado.
“The day that my son died, I was 21 weeks and five or six days,” Lynn said. “And that was only because we were able to get appointments back-to-back; that’s so incredibly highly unusual.”
Lynn said she knows people who’ve had normal scans at 20 and 22 weeks only to face tragedy. “And then, bam, at 24 or 25 weeks, all of a sudden the [fetus’] brain matter is gone and their skull is full of fluid. And those families would be left with absolutely zero option” if Colorado voters approve the ballot measure, Lynn said. “To be blunt, they’re screwed.”
Colorado is one of seven states that doesn’t have a gestational limit on abortion care. Proposition 115, which mirrors a Colorado House bill that failed in committee this session, is a citizen-led ballot initiative that would create a state law banning abortions after 22 weeks except when the pregnant person’s life is immediately threatened. It has no exceptions for fetal anomalies or pregnancies resulting from rape or incest.
People have later abortions for several reasons: fetal anomalies diagnosed in the second and third trimesters, life-threatening pregnancy complications, pregnancies resulting from rape or incest, and logistical or financial barriers to getting care in hostile places like Texas and Louisiana that push pregnant people past the gestational limit in their state.
Proposition 115 is Colorado’s fourth anti-choice ballot initiative in 12 years. The previous three, efforts to establish fetal “personhood” in the state constitution, were roundly defeated. After those failures, anti-abortion lawmakers and activists refocused on a new type of ban that could potentially succeed with voters, said Elisabeth Smith, chief counsel for state policy and advocacy at the Center for Reproductive Rights.
Organizers of the ballot initiative call it a “reasonable limit” on abortion. But providers, patients, and advocates point out that an arbitrary ban is harmful and cruel.
“I cannot convey enough how medically inappropriate a one-size-fits-all, line-in-the-sand ban is,” said Dr. Kristina Tocce, medical director at Planned Parenthood of the Rocky Mountains. “Every patient and every pregnancy is unique, and care needs [to be] individualized.” Further, some pregnancies will never be viable, Tocce said.
Dusti Gurule, executive director of Colorado Organization for Latina Opportunity and Reproductive Rights (COLOR), the state’s only Latina-led reproductive justice organization, urged people to consider the lives of those who will be hit hardest if Proposition 115 passes.
“At the end of every policy decision is a person who lives with it, who makes the decision with their families, friends, medical providers,” she said.
The impact of abortion bans fall hardest on women of color, who are paid less than white women and are more likely to lack health-care coverage in the first place, Gurule noted. People who have low enough incomes to qualify for Colorado’s Medicaid program already cannot use their insurance for an abortion. The obstacles to getting care can multiply: possible language barriers, no paid time off work, lack of transportation, childcare for kids they may already have, fear of seeking care due to anti-immigrant rhetoric.
Empathetic people should be able to understand why someone wasn’t able to afford an abortion until 22 weeks, Gurule said. “We can’t assume that people are living a life as easy as maybe it is for some of us.”
‘Place of last resort’
If Colorado residents had to travel out of state for later abortions, the costs would only increase, putting care out of reach for many.
Dr. Warren Hern, whose Boulder Abortion Clinic has operated since 1975, is the only Colorado provider specializing in later abortion care. Hern said he treats people from all over the United States; about ten percent of his patients are from Canada, while others come from Europe. In mid-September, his clinic cared for a woman from Australia.
“These are complicated situations, and people who have nothing to do with the patient have no business interfering with their access to abortion care,” Hern said. “A lot of people think, ‘Oh, it’d be reasonable to limit abortion [after 22 weeks].’ Well wait a minute, this ignores the woman’s situation, and the anti-abortion people make it all about the fetus, which they call a baby, an unborn child, which of course it’s not. … I think that they see the woman as simply a passive vessel for the fetus.” He called Proposition 115 a “repressive, totalitarian measure.”
While the personhood amendments were easily defeated, Hern said he’s worried about this vote since many don’t know the reasons why people need abortions later in pregnancy.
“Unless people understand how bad it is, the anti-abortion religious fanatics will go out in droves and get it passed,” Hern said. “We need to help people understand why it’s so critically important for women to be able to make this choice.”
Karen Middleton, president of Cobalt (formerly NARAL Pro-Choice Colorado), said the advocacy group is trying to educate voters on both why people have later abortions and why the opposition is targeting Colorado specifically—and using misleading tactics to do it.
“For people all over the country, this is often their place of last resort,” Middleton said. Anti-choice activists’ “big-picture political scheme is to shut off access in states where abortion care is available to try to eliminate access to abortion altogether.”
Three Colorado women who’ve had later abortions said they’re angry that anti-choice activists are politicizing the difficult decisions they made and trying to interfere with people’s health and lives.
Rhonda Pohlman, who ended her nonviable pregnancy in 2006 at 21 weeks and six days, called Proposition 115 “absolutely terrifying.” Her son had a large cyst separating the two halves of his brain, and she was told that he would likely suffocate in utero. If the 22-week ban were to become law, then in cases like hers, the state would essentially be taking the position of “too bad, but we’re just gonna let the baby die in utero and then hope to god you don’t get sick,” she said.“These are complicated situations, and people who have nothing to do with the patient have no business interfering with their access to abortion care.” -Dr. Warren Hern
Pohlman is a pharmacist, but she said that even with a medical background, she had to read the text of the ballot measure two or three times before understanding it. She worries that voters will glance at it and vote yes.
“If they just look at the surface and they don’t think of the decisions that go into it, and the people that they potentially are affecting, I absolutely can see how people will be like, ‘Oh, well yeah this [proposition] makes total sense,” she said.
Lynn noted that a ban on later abortions with no exception for fetal diagnoses would be unspeakably cruel for visibly pregnant people interacting with well-meaning strangers asking about due dates and the baby’s sex.
“To have that happen knowing that my baby is dying would add just an incredible level of trauma—I can’t even explain that,” Lynn said. “I would not have wanted to leave my house, I would have become a hermit.”
Even in cases that don’t involve fetal anomalies, Lynn said people have ideas about later abortion that are detached from reality. In fact, these procedures are difficult to schedule and astronomically expensive. Plus, she pointed out how anti-choice clinics, commonly known as crisis pregnancy centers, mislead people by giving them incorrect gestational ages or telling them they have lots of time to make a choice.
“No decision to have an abortion, especially later in pregnancy, is taken lightly,” Lynn said. “And the further along you are, the more expensive that procedure is. It’s not $500 or $600 at the local Planned Parenthood—it’s $10,000 to $25,000 at a clinic out of state. That’s a huge amount of money.” People are not waking up 30 weeks into pregnancy and deciding they want an abortion.
If Christina Taylor had still lived in Texas when she learned at 20 weeks pregnant that the fetus she was carrying had no kidneys or bladder and there was no amniotic fluid in her uterus, she wouldn’t have been able to have an abortion in her state. She would have had to travel or continue carrying the pregnancy until the fetus was likely crushed by her organs, her doctor told her.
But she had moved to Colorado a few years prior and was able to have an abortion at 21 weeks. So many things fell into place: She got second-opinion appointments immediately, her insurance covered the procedure, and her retired mom could come take care of her other kids.
“It really scares me that they have this [proposed ban] at 22 weeks,” Taylor said. Though she is Latina, she acknowledges some privileges from being middle class and seeking this care alongside her white husband. She sees how barriers to abortion could put care out of reach for other people who look like her.
“I am very able to imagine if my life was a little bit different, how much more difficult this would be—having financial ability to do this, having the insurance, having the family support,” Taylor said. “It could be so much worse.”
Taylor said she has a certain level of guilt knowing later abortion in the case of a nonviable pregnancy is “the more palatable one” to some voters, but she doesn’t think her abortion is any more justified than anyone else’s; she fully supports other people’s freedom to choose when or when not to be pregnant.
Preparing for the worst-case scenario
If Proposition 115 were to pass, it could have ripple effects far outside of Colorado. For one thing, people out of state travel there for abortions later in pregnancy; any federal lawsuits challenging the measure could lead courts to revisit the central holding of Roe v. Wade: that states can’t ban abortion before fetal viability, thought to be around 24 weeks.
Cobalt is doing everything it can to get people to vote no, including text banking, phone calls, mailers, digital ads, and several weeks of TV ads. Still, if the proposition succeeds, the group’s abortion fund has become more nimble during the COVID-19 pandemic by helping people with practical support like rides and grocery deliveries. Middleton acknowledged that as a worst-case scenario the group would help people try to get care nearby. (Neighboring New Mexico is one of the other states without a gestational limit.)
COLOR plans to contact close to 200,000 Latinas and their families by phone and mail to educate voters about abortion later in pregnancy and explain why states shouldn’t be banning any kind of health care.
If Proposition 115 were to pass, Gurule said COLOR would be interested in challenging it and even bringing the issue back to the ballot if necessary. But the group, she added, would also support abortion funds to help people who would need to leave the state to get care.
If the measure passes, legal challenges will be fraught.
“We’re in a very precarious position,” Smith said. Following the death of liberal Justice Ruth Bader Ginsburg, “we are potentially looking at a 6-3 majority on the court of justices opposed to abortion rights.”
While 22 weeks is before fetal viability and any abortion ban at that point is thereby unconstitutional, “we get back to the question of what the Supreme Court will look like and who will fill Justice Ginsburg’s seat,” Smith said. Depending on what happens with the Court, advocates might choose to challenge the law at the state rather than federal level.
Middleton said the makeup of the Supreme Court gives her pause on whether Cobalt would challenge a successful ballot measure. But Hern, the Colorado doctor who provides later abortion care, pledged to fight the ban if it passes: “I will be there with attorneys to challenge this in court on the first day.”
The American Medical Association is asking the Supreme Court to strike down a Trump administration rule that’s had a far-reaching impact on the nation’s family planning program
WASHINGTON — The nation’s largest doctors’ group on Thursday asked the Supreme Court to strike down a Trump administration rule that’s had a far-reaching impact on family planning by prohibiting taxpayer-funded clinics from referring women for abortions.
The American Medical Association acted after two U.S. appeals courts issued conflicting rulings on the legality of the Trump administration restrictions, which apply to clinics that mainly serve low-income women.
“We do think this conflict needs to be resolved and we need to figure out how to deliver services under a program that has had bipartisan support for decades,” said AMA President Dr. Susan Bailey.
The AMA’s move will raise the profile of a reproductive rights issue overshadowed by bigger election-year battles. The recent death of liberal Justice Ruth Bader Ginsburg has prompted speculation that a more conservative court could overturn the Roe v. Wade decision that legalized abortion, as well as the Obama health law that expanded coverage and made birth control free for most women.
But the changes to Title X, as the federal family planning program is known, are already in effect — and getting much less attention.
Last year the Trump administration finalized a rule that prohibits clinics from referring pregnant women for abortions and imposes other restrictions, including a requirement for strict financial and physical separation of family planning facilities from ones that provide abortions.
As a result, more than 900 out of nearly 4,000 clinics receiving federal funds left the program, including Planned Parenthood and its affiliates. Advocates say the exodus has disrupted care for women who receive birth control and routine medical attention from the clinics. The program usually serves some 4 million clients, and the AMA says that was down about 20% last year.
The Trump administration’s regulation “warps and decimates” Title X, the AMA said in its petition asking the Supreme Court to take the case.
An appeals court based in San Francisco upheld the Trump administration’s regulations, but a second court based in Richmond, Virginia, ruled in a Maryland case that the restrictions were invalid. The AMA says that means the administration’s abortion referral rule is in effect everywhere but Maryland.
Casting the case as an issue of free speech and medical ethics, the AMA said the administration’s rule attempts to control communication between clinicians and patients by prohibiting abortion referrals, while at the same time compelling clinics to refer pregnant women for prenatal care, even if a woman has decided that she wants to have an abortion.
“The patient-physician relationship is the cornerstone of good medical care, and patients must be able to believe and completely trust that their physicians are giving them all of their options, and that communication is not being blocked in any way,” said Bailey. “It is frankly against our code of medical ethics.”
In response, the Health and Human Services department rejected the accusation that the regulation amounts to a “gag rule” and noted that the federal appeals court in politically liberal San Francisco upheld it. Nonetheless, it was a conservative mix of appellate judges who decided the case.
HHS also says it is trying to increase the number of patients served and improve quality.
Longstanding laws prohibit the use of federal funds to pay for abortions, but the family planning rule is part of a broader Republican effort to shut down various streams of taxpayer money still available to Planned Parenthood, the nation’s largest provider of abortions. That’s been a critical priority for religious and social conservatives in President Donald Trump’s political base.
Abortion remains a legal medical procedure, but the number and rate of abortions is at its lowest point in nearly 50 years. Improved access to birth control is seen as one of the reasons.
Democratic presidential candidate Joe Biden promises to rescind the Trump administration’s family planning rule and also supports allowing federal programs to pay for abortions. But the AMA says regardless of who wins the election, it believes the Supreme Court should address the issue and overturn the Trump administration rule.
“Title X has contributed to a 30-year low in unintended pregnancies,” said Bailey. “We can’t afford to walk away from that progress.”
Joining the AMA’s petition are the ACLU, Planned Parenthood, the National Family Planning & Reproductive Health Association, and Essential Access Health, which administers the Title X family planning program in California.
President Donald Trump filled the first presidential debate of the 2020 general election with a collection of lies often heard on Fox News, including about the future of legal abortion access. Despite his contrary past comments on the issue, Trump falsely claimed during the debate that his Supreme Court nominee, Amy Coney Barrett, would not pose a threat to Roe v. Wade.
His statement came after Democratic presidential nominee Joe Biden said Trump’s opposition to Roe is “on the ballot” and “at stake right now” with the nomination of Barrett. Trump jumped in multiple times to claim the issue of Roe was “not on the ballot” with Barrett and that Biden doesn’t “know her view on Roe v. Wade.”
Trump is lying. As CBS’ Kate Smith tweeted, Trump’s injections are “interesting and a little confusing” because he has repeatedly said he would appoint justices to the court who would overturn Roe. During the 2016 presidential debates, moderator Chris Wallace asked Trump, “Do you want to see the court overturn Roe v. Wade?” Trump responded, “Well, if we put another two or perhaps three justices on that’s really what’s going to be — that will happen. That will happen automatically in my opinion.”
By now, this is a tired, worn-out strategy by Trump — he did it with both Neil Gorsuch and Brett Kavanaugh, as NPR’s Ron Elving noted back in 2018. As Elving wrote then, “The apparently mixed signals of the moment do not really suggest any further evolution in the president’s thinking. They suggest a strategy for confirming whomever the president picks.”
On The Daily Wire’s The Ben Shapiro Show, Shapiro said that if Barrett is confirmed, “the chances of Roe v. Wade being overturned are nearly zero. I say nearly zero only because I hedge my bets a little bit. They are basically zero. Roe v. Wade is not going to be overturned.”
On Fox News’ America’s Newsroom, The Wall Street Journal’s Bill McGurn claimed, “Even if Roe v. Wade were overturned, which I do not think it will be, at least in its entirety, you know, abortion would still be legal and up to the states. So, I don’t think we’re gonna see any cataclysmic changes.”
National Review’s Andrew C. McCarthy wrote, “No Supreme Court appointment by a Republican president would be complete without the Left’s obligatory hysteria about the purportedly imminent demise of Roe v. Wade.” He claimed, “The Supreme Court would almost certainly decline to review” a case of a state banning abortion, adding, “This is not a sure thing, but I suspect it is close to sure, much as I personally wish it were not.”
On Hannity, Fox News host Sean Hannity said, “On the issue of abortion, in spite of the lies the left will tell you, Judge Barrett has been described as personally pro-life but has expressed doubts that Roe v. Wade will ever be overturned.”
On Fox & Friends Weekend, Fox contributor Robert Jeffress claimed, “As long as the majority of Americans favor abortion of some kind, they are not going to overturn Roe vs. Wade.”
Jeffress’ comment in particular reveals the why behind this strategy. An overwhelming majority of Americans supportRoe and don’t want it overturned. If it weren’t so popular, abortion opponents wouldn’t be forced to mask their intentions and hide behind the talking point that it won’t be overturned. As MSNBC’s Steve Benen wrote about Ernst’s lie about Roe:
It’s likely that the GOP senator, like others in her party, simply hope Americans don’t fully realize the consequences of what the party is about to do — because if voters recognized how much society is poised to change as a result of an even-more-conservative Supreme Court, Republican officials and candidates would face an even more challenging electoral landscape in 2020.
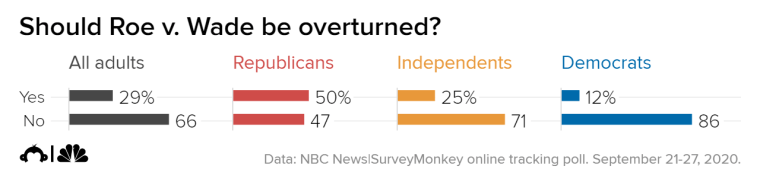
Sixty-six percent of adults say they don’t think the Supreme Court should overturn Roe v. Wade, according to an NBC News|SurveyMonkey Weekly Tracking poll.
Abortion rights activists protest outside the Supreme Court on March 4.Saul Loeb / AFP – Getty Images
A majority of American adults say they don’t support the Supreme Court’s completely overturning Roe v. Wade, according to new data from the NBC News|SurveyMonkey Weekly Tracking Poll.
Sixty-six percent of adults say they don’t believe the Supreme Court should completely overturn the decision that established a woman’s right to an abortion nationwide in at least the first three months of a pregnancy. Twenty-nine percent of adults say they do want the court to completely overturn the ruling.
The landmark 1973 decision found that a woman’s constitutional right to privacy protected her choice of whether to have an abortion, although it also allowed states to more heavily regulate access to abortion after the first trimester. Before Roe v. Wade, states were largely unrestricted in regulating access to abortion at any point in a pregnancy.
Democrats are overwhelmingly in favor of preserving the decision — 86 percent say it shouldn’t be overturned, while 12 percent believe it should be overturned.
Independents feel similarly — 71 percent want to preserve the ruling, while 25 percent want to see it overturned.
Republicans are virtually split, with 50 percent supporting overturning Roe and 47 percent saying it shouldn’t be overturned.
In a 2013 article in the Texas Law Review, Barrett cited Roe v. Wade when she wrote, “If anything, the public response to controversial cases like Roe reflects public rejection of the proposition that [precedent] can declare a permanent victor in a divisive constitutional struggle rather than desire that precedent remain forever unchanging.”
Barrett, however, has said that she doesn’t believe the Supreme Court would ever fully overturn abortion rights — rather that the court may change how much power states have to regulate abortions.
In a speech at the University of Notre Dame in 2013, Barrett said, “The fundamental element, that the woman has a right to choose abortion, will probably stand.” And in 2016, she said: “I don’t think abortion or the right to abortion would change. I think some of the restrictions would change.”
After he nominated her, Trump said in a “Fox and Friends” interview that with Barrett on the court, overturning Roe v. Wade was “certainly possible.”
“And maybe they do it in a different way. Maybe they’d give it back to the states. You just don’t know what’s going to happen,” he said.
Many conservatives have pushed for the court to re-examine Roe — Sen. Josh Hawley, R-Mo., tweeted this month that he would vote only for Supreme Court nominees who believe “Roe was wrongly decided.”
The new data tracks with other polls that show that the majority of Americans don’t want to see Roe v. Wade completely overturned and generally agree with a women’s right to have an abortion with certain restrictions.
The timing of Barrett’s nomination is also controversial. Last week, a Washington Post/ABC News poll found that 57 percent of Americans thought the candidate who wins the Nov. 3 election should fill the vacant seat. And two NBC News/Marist College polls showed that a majority of likely voters in Michigan and Wisconsin agreed that the election winner should make the nomination.
The chair of the Senate Judiciary Committee, Lindsey Graham, R-S.C., announced that Barrett’s confirmation hearings would begin Oct. 12 — just 22 days before the election. Democrats have criticized Republicans for moving forward with the nomination and the confirmation process so close to the election after having blocked President Barack Obama’s nomination of Merrick Garland in March 2016.
While Democrats have promised to try to block Barrett’s confirmation, only two Republican senators — Susan Collins of Maine and Lisa Murkowski of Alaska — have joined with them to say a nominee shouldn’t be confirmed until after the election, so there’s little that Democrats can do to delay the process.
A federal judge has temporarily blocked a Tennessee abortion counseling requirement, the logic of which doctors and health care providers say is not supported by science, days before it was slated to go into effect.
A July law required Tennessee abortion providers to tell abortion seekers that medication abortion — a nonsurgical procedure effective until about 10 weeks into a pregnancy that typically entails taking two drugs several days apart — can potentially be reversed. The law also required that information about the procedure be made available on the state’s department of health website, and that providers inform patients of it.Such requirements have been widely criticized by medical groups, and researchers in California stopped a 2019 trial designed to study the “abortion reversal” treatment early due to safety concerns.
The American Medical Association — the main industry group for doctors, which sued North Dakota over a similar law in 2019 — has called such claims about medication abortion reversal “wholly unsupported by the best, most reliable scientific evidence.” The American College of Obstetricians and Gynecologists has stated that “medication abortion ‘reversal’ claims are unsupported by science,” criticizing “legislative mandates forcing physicians to steer women to this unproven course of treatment.
“This win for abortion rights supporters comes as both sides of the abortion rights debate gear up for a Supreme Court fight over nominee Judge Amy Coney Barrett to replace the vacancy left by the late Justice Ruth Bader Ginsburg. Confirming Barrett, who has expressed views at odds with abortion rights and would cement a 6-3 conservative majority on the court, could have profound implications for the future of abortion rights.
Tennessee’s law would require such warnings from the physician at least 48 hours before the abortion, again in writing after the first pill has been administered, and written on “conspicuously” displayed signs in private offices, ambulatory surgical treatment centers, facilities and clinics that have provided more than 50 abortions in the previous calendar year. Violating the statute could land abortion providers with up to six years in prison and health centers with a $10,000 fine.
Tennessee abortion providers, joined by Planned Parenthood, the American Civil Liberties Union and its Tennessee affiliate, and the Center for Reproductive Rights, challenged the law in August, suing Tennessee Republican Attorney General Herbert Slatery and other Tennessee officials for compelling them to issue “untruthful, misleading, and irrelevant information.
“Judge William Campbell wrote Tuesday that he was “unable to assess fully the competing expert opinions as to whether the mandated message is ‘truthful and not misleading,’ in the absence of the experts’ testimony,” but found that “another aspect of the mandated message is ‘misleading.’ “He noted that because abortion providers would have to start conveying that abortion reversal information was on the department of health website starting October 1, but the deadline for the state department of health to post the information was January 1, “such information and assistance may not be available” such that “a patient desiring to access such information would be unable to do so.
“Campbell noted that “plaintiffs have demonstrated a strong or substantial likelihood of success on the merits of their claims that (the set of requirements) violates the First Amendment by requiring abortion providers to convey a mandated message that is misleading.” The block on the law will last until October 13, the date for which Campbell has scheduled a hearing in the case.
Slatery’s office said in a statement to CNN Wednesday that Campbell’s order “merely preserves the status quo until the district court can hold a preliminary injunction hearing,” adding that “we look forward to presenting evidence at the hearing to support the constitutionality of the statute.
“Ashley Coffield, CEO of plaintiff Planned Parenthood of Tennessee and North Mississippi, cheered the “victory in blocking another failed policy” while slamming “how anti-abortion politicians carry out the Trump administration’s agenda against our rights and freedoms — without public input and against the will of the people.
“Tennessee is not alone in pursuing such a law of late. Arkansas, Kentucky, Nebraska, North Dakota and Oklahoma all codified measures in 2019 year requiring abortion providers to tell patients that medication abortion could be reversed. A federal judge blocked the North Dakota law last year.
And medication abortion reversal isn’t the only facet of the procedure the state has looked to regulate. The law mandating the abortion reversal notice requirement also looked to ban abortions after a fetal heartbeat is detected, which can occur as early as six weeks into a pregnancy and before many people know they’re pregnant. Campbell also temporarily blocked that provision in July.
While people worry about a world in which abortion access is no longer protected, the women of Mississippi are already living it.
“I would drink bleach right now.”
Kate shakes her head, and her long, sun-streaked brown hair, piled high in a messy bun, shivers. “That’s so bad, and I don’t mean it,” she quickly adds.
She’s exhausted; shadowy crescents frame her bright eyes. Just a few weeks ago, she graduated from the University of Mississippi. “My one goal, as pathetic as it sounds, was do not walk across that stage pregnant,” she says. “Everything I worked for…I’m going to remember graduating and being pregnant.” Kate has been trying to get an abortion since March. It’s a Friday evening at the end of May, and she was just turned away from an Arkansas clinic, about 200 miles from home.You can also listen to Becca Andrews’ story read aloud:https://audm.herokuapp.com/player-embed/?pub=mojo&articleID=roe-doesnt-reach
In the morning, she’ll have to go back home to Oxford, Mississippi, where she’ll wait yet another week, and return to the clinic in Little Rock for the third and hopefully final time.
Her day began at 3 a.m., with a text from Laurie Bertram Roberts. Roberts helms the Mississippi Reproductive Freedom Fund, the nonprofit that was helping Kate get her abortion. Around 7:45 a.m., a white medical transport van arrived at her apartment, and Kate climbed in to join two of Roberts’ daughters, Sarah and Aolani, as well as Roberts’ partner, who was driving but did not want to be named. The crew journeyed northwest, through Mississippi, then Tennessee, then Arkansas. Traffic on the interstate slowed them down; by the time they made it for her 10:45 a.m. appointment, it was nearly noon.
Kate at home.
Tired and dusty—the van’s air conditioning was broken, so the windows stayed down—the foursome stepped out into the humid Arkansas air. About 15 protesters hemmed in the clinic, and Kate kept her head down as a man bellowed that God would not judge her, if only she would turn around. Another protester, a woman with an infant, shrieked that Kate should carry to term and give the baby to her. It was that image—the baby nestled in the stroller, in the edge-of-June heat—that Kate says was seared into her mind the rest of the day.
After rushing into the clinic cocooned by her companions, Kate faced the metal detector, putting her wallet in a dish. The strict security was jarring the first time she visited, even though it’s pretty typical in clinics. Still, she couldn’t bring herself to unclasp the vintage necklace she almost never takes off; she breathed a sigh of relief when it didn’t trigger the alarm. Her cellphone was left in the van—another security measure, meant to protect patient privacy and stymie anti-abortion activists who pose as patients and film inside clinics—making her feel even more alone. She hadn’t told her mother, who was battling a serious illness, about her pregnancy, or her new boyfriend. Just about everyone she had told was in the clinic with her.
Kate’s memory of the rest of the appointment is blurry. She remembers some complication with payment and a sharp admonishment from an administrator about her tardiness, which brought forth the tears she had successfully held in until then. Called back to the exam room, she was relieved to see her favorite clinic staffer there. At a prior appointment, the staffer had made Kate feel comfortable and reassured. But now, performing the ultrasound, the energetic, warm woman grew quiet. “What’s wrong?” Kate demanded, her body tightening with fear.
Early morning in Mississippi.
“Oh, things are just going to go a little differently today,” the staffer replied, trying to keep her tone light. Kate clenched her jaw against the rising bile in her throat.
The ultrasound was showing the fetus at 20 weeks, but Kate’s appointment was for someone who was 18 weeks along. That meant Kate couldn’t get her abortion. The extra two weeks triggered a 48-hour waiting period and state-mandated counseling about fetal pain—a concept that’s been widely debunked for more than a decade. She would have to make the journey all over again for an appointment next week. That would be her final chance to get the procedure in Little Rock; abortions after 22 weeks are illegal in the state. It was already too late to get one in Mississippi, where abortion is not available after 16 weeks.
As a nurse explained the situation and began the required monologue about fetal pain, Kate’s eyes filled with bright white light, and she gagged.
I first meet Kate, a pseudonym to protect her identity, by the pool at a Little Rock hotel a few hours after she was turned away by the clinic. Her fingertips are stained bright orange-red, courtesy of a bag of Flamin’ Hot Cheetos, and she is wearing the summertime uniform of college girls in the South—oversize T-shirt, athletic shorts, sandals. She greets me with a warm familiarity and says she hopes I can explain what just happened to her, because she has been too afraid to Google much of anything.
Kate tells me repeatedly that she’s passionate about helping people. She wants kids someday, with the right person. The man who impregnated her is not that. They were only sexual the one time; she had been drinking and she doesn’t remember how they ended up at her apartment that night. When she told him she was pregnant and that she wanted an abortion, he said it was her choice.
Kate worried she would be judged if she went to the clinic in Jackson—the only one in the state. “Ole Miss is apparently the most liberal area in Mississippi, and it is not open-minded,” she says. It took her some time to find an alternative, sifting through search results for crisis pregnancy centers—anti-abortion establishments that aim to convince women to carry to term based on religious conviction. She called a legitimate abortion clinic in Memphis, but the receptionist sounded overwhelmed, and it made Kate’s anxiety swell. Finally, she made an appointment in Little Rock for early March.
The man who impregnated her drove her to the clinic that day, and he promised to pay for her procedure, Kate says. They were in the car by 4 a.m.; Kate wanted an early appointment so she could make it back in time for a night class. She was later surprised when the clinic asked for payment upon her next visit. Apparently, the man declined to pay for the appointment while she was in the exam room.
He later asked Kate to keep the baby and give it to him. She refused. The morning of her third appointment, she found her tires slashed. That’s when she decided she needed help. That’s when she found Laurie.
Laurie Bertram Roberts’ life is chaotic. A 41-year-old woman with seven children, she lives below the poverty line. Her family cobbles together a modest life with the help of food stamps, government assistance, and the odd jobs they do to survive. Roberts spends much of her time bedbound due to painful fibromyalgia, but her phone and laptop are never far, basically operating as digital appendages. As a co-founder and the executive director of the Mississippi Reproductive Freedom Fund, the only abortion fund in the state, Roberts has run an organization for the past six years that’s neither seamless nor neatly organized, but it is powerful. Its budget grew to $110,000 this year and it helps at least 10 or so individuals each month get abortions, sometimes smuggling those in abusive relationships out of their homes for the procedure.
Laurie Bertram Roberts, co-founder of Mississippi Reproductive Freedom Fund orders books for their lending library while recovering from a sinus infection.
The fund doesn’t just pay for abortions and coordinate logistics. Roberts, a woman of color, is a true believer in the reproductive justice framework—a term coined by a group of black women in the ’90s, detailing, as their organization now puts it, the “human right to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.” The Mississippi Reproductive Freedom Fund helps women pay for health care, diapers, food, contraception—wherever there’s a need, the fund will fill it. Roberts delightedly shows me several boxes of Barbies, in every shape, size, and color, that she purchased for a playroom for her clients’ children. “No one comes to us just needing one thing. Needing abortion funding is usually one part of their greater struggle of being a low-income person,” she says.“I don’t think [outsiders] understand that the structural barriers are at every turn of care, that it starts before people even have sex,” Roberts says.
When I visit the house in West Jackson where Roberts lives and eventually plans to host clients overnight, it is teeming with activity. The one-story “fundshack,” as she and her family call it, is modest, with a front porch framed by lacy white iron posts, shot through with rust, and bars clamped protectively over the windows. Roberts’ daughters Kayla, Sarah, and Aolani—who grew up with social justice at the center of their lives the way most kids here grow up with religion—drift in and out, as do local activists from youth empowerment and LGBTQ organizations. An unexpected donation of several mattresses is delivered, while fund volunteers intermittently pop into the room where Roberts sits in bed, chatting with me, her lower half wrapped in a blue sheet. Roofers work in the hot sun to replace the worn-down shingles. Roberts tells me it took her a few tries to find a reliable crew who didn’t mind working for a group that funds abortion care and were willing to work in a poor “black” part of town. She seems to have hit it off with these guys. A day or two prior, the subject of condoms came up when she was talking with them, as it tends to around Roberts, and soon enough she was using a wooden penis to demonstrate how to properly put one on. She says the men left that day with a generous bag of free condoms.
“I’m very plainspoken about sex,” she says, shrugging.
Roberts is actually plainspoken about almost everything—she doesn’t much care for bullshit, and she’s not afraid to let you know it. She knows firsthand there are worse things than appearing abrasive: like being denied an abortion when your back is against a wall. Like nearly dying in a Catholic hospital because the doctor is more interested in saving the fetus than the woman with children at home. Like being a low-income woman of color in a state with a long record of denying the humanity of those who look like you. All of these factors, all this personal history, contribute to why she’s doing this work and why it is messy and frenzied—such is the life of someone who lives with the odds stacked against them, and such are the lives of those who come to her for help.
The Mississippi Reproductive Freedom Fund in Jackson, Mississippi.
“We’re all poor women and femmes and people of color, for the most part. We have a couple of low-income queer white folks working for us,” she says. “To be part of our leadership, you have to be a low-income or working-class person, period. We’re not apologetic about that at all, and we’re unapologetically black as fuck. You can either rock with it or kick rocks, we don’t care.”
That’s a revolutionary attitude for Mississippi, the state with the second-highest poverty rate in the nation, where, in many ways, post-Roe America is already a reality. In a study of 47 states there were 11.8 abortions per 1,000 women of reproductive age in 2015, but in Mississippi there were just 7.8. Even so, a year earlier an estimated 47 percent of all pregnancies in the state were unintended, while nationally it was 41 percent. Also, in 2017, Mississippi’s birthrate among 15- to 19-year-olds was 65 percent higher than the national average.
In recent years, the state has twice attempted to place a severe gestational limit on abortion—first, a 2018 law that would have banned abortions after 15 weeks, and this past May, another law that would have banned abortions after six weeks. The measures were signed by Gov. Phil Bryant, who famously said his “goal is to end abortion” in Mississippi, but a federal judge struck down or blocked the laws.
The Jackson clinic’s capacity has been slowly whittled down by an onslaught of legislative attacks—it’s now only open three days a week. It is required to meet the onerous standards of an ambulatory surgical center. The state mandates every patient undergo medically inaccurate counseling and be subjected to an ultrasound and a 24-hour waiting period, which means two separate trips to the clinic. Nearly half of Mississippians seeking abortion care travel out of state to get it, but even then, its neighbors in the Bible Belt aren’t much better off. While Tennessee has seven clinics operating as of recently, Alabama and Louisiana have just three each, and Arkansas was down to two this summer. These states feature a patchwork of Targeted Regulation of Abortion Providers (TRAP) laws, policies aimed at limiting access to abortion care through seemingly harmless provisions about hallway widths or expensive medical equipment unnecessary to abortion.
Low-income women suffer the most in the state’s abortion desert, making Roberts’ job all the more crucial. According to 2017 data from the Kaiser Family Foundation, more than 1 in 10 women in Mississippi receive health care coverage through Medicaid and likely can’t afford to pay for an abortion or nonemergency contraception on their own. In 2016, the state health department closed nine clinics; the following year, two-thirds of the department’s regional offices were shuttered due to a series of budget cuts. According to Roberts, some women she knows who rely on Medicaid have had to wait up to six months to get birth control. The state has a single Planned Parenthood, in Hattiesburg, that distributes birth control but does not provide abortion care—which, according to Barbara Ann Luttrell, director of communications for Planned Parenthood Southeast, “is because the state of Mississippi intentionally has made it next to impossible to be an abortion provider.” Planned Parenthood Southeast is also one of the most under-resourced affiliates in the country.
Aolani Jefferson outside the Mississippi Reproductive Freedom Fund.Sarah Roberts, abortion doula and daughter of Laurie Bertram Roberts, at the Mississippi Reproductive Freedom Fund.
“I don’t think [outsiders] understand that the structural barriers are at every turn of care, that it starts before people even have sex,” Roberts says.
Roberts wishes her fund could overcome some of these obstacles by helping women like Kate manage their own abortions at home, in peace—largely with medication abortion. She sees misoprostol and mifepristone as equalizers for anyone seeking an abortion, particularly rural women who live hundreds of miles from a clinic. But in Mississippi and 33 other states, it is a crime to use medication to induce an abortion if that medication is not administered by a licensed clinician. Mississippi also bans the use of telemedicine, in which doctors see a patient remotely, despite a 2017 study finding that telemedicine is as safe as an in-person doctor visit for medication abortion.
Above all, Roberts fears what seems like the next big battle in the war on abortion: criminalizing women by giving fetuses the same rights as people. This is already happening, most frequently when pregnant women use drugs. While Mississippi doesn’t have a law that criminalizes drug use while pregnant, prosecutors in at least one county, Jones County, have fashioned a loophole through which approximately 20 women have been charged under a “felonious child abuse statute”—reasoning that if a woman uses drugs, she is poisoning the fetus, and therefore is criminally liable. Roberts has put up bail for one woman who was jailed under the statute. “I knew Jones County was bad when we called the bail bondswoman to get her out, and the bail bondsperson told me, ‘I’m so glad y’all are helping her, because I have so many women that I bail out every year in her same situation and it’s horrible, it’s ridiculous, and someone needs to stop it,’” Roberts says, laughing darkly. “Bail bondspeople aren’t usually on the side of the people they’re bailing out.” Roberts also got involved in a widely publicized case in Alabama, in which a black woman named Marshae Jones was charged with manslaughter when she was shot in the stomach while pregnant. Though the charges were ultimately dropped, Roberts helped a local abortion fund raise money to pay Jones’ bail and hire a lawyer.
Despite this excruciating landscape, Roberts is proud that Mississippi is where she came into her own—it’s where she fled her abusive partner when she was 27; it’s where she went to college; it’s where she raised her kids. It’s where she grew into a hellraising activist, surrounded by other activists, many of whom had a history in the civil rights movement. It was the first place in her life where she found herself in a majority-black space. “I generally talk about Mississippi being the Broadway of activism,” she tells me. “If you can make it here, you can make it anywhere.”
Kate spends most of the journey home from Little Rock curled up on the floor of the van. She hadn’t been sleeping much since she found out she was pregnant a few months ago, and last night was no better. After lunch, Sarah and Aolani stop at a Walmart for a thin foam mattress pad and a cheap tie-dye blanket to make a bed for Kate. As the van hurtles down the interstate, Roberts’ partner behind the wheel chugs energy drinks, slinging expletives out the window every so often at other motorists. Air roars through the open windows, and a vent in the top of the van clatters, making it impossible to talk much. Kate quietly lies there, occasionally picking up her phone only to set it back down. Sweat has pasted her two-sizes-too-big T-shirt to her back, and the folds of the blanket have left creases on her legs. Sarah passes her phone around every so often to share an amusing Tumblr meme. Kate humors Sarah, but her smile hardens into more of a grimace.
“I can’t believe I have to do this all over again in a week,” Kate mumbles as we wait to use the restroom in a grimy gas station near the Tennessee state line. She is eager to see her dog, who has been her devoted companion throughout this ordeal, sleeping in the bathtub on nights when Kate was too sick to move from the toilet. When we pull into her apartment’s parking lot, she tries to quickly exit the van but has to wait for a nosy neighbor to go inside. “Let us know if you need to talk,” Sarah calls after Kate.
As I watch Kate hurry away, I wonder if she’ll be able to steel herself to repeat the trip. I would have understood if she couldn’t; she had pushed through a series of grueling obstacles only to be met with still more. But less than a week later, on a rainy Thursday morning, the group began the process all over again. This time, Kate got her abortion. If she had waited even a few days longer, she would have been rendered ineligible for the procedure, which would have meant a journey to Florida or Colorado. What’s more, if she had started this arduous process just a few weeks later, she might not have been eligible for an abortion in Arkansas at 20 weeks. This year, legislators passed a law banning abortions past 18 weeks there, shaving four more weeks off the window for the procedure, but its opponents sued the state and a federal judge has temporarily blocked it from going into effect.
When we speak a few days after the abortion, Kate sounds lighter. She says she finally feels calm and ready to move forward. She’s considering a couple of internship options, one of which would take her out of Mississippi altogether. “When I got into my apartment, I literally just laid down with [my dog], and finally, I felt like I had a sense of control again.”
The sun rises on a church in Oxford, Mississippi.Coldwater, Mississippi.
wonder when the IUD tweets are going to start,” I texted to a friend on Sept. 18, the night that Justice Ruth Bader Ginsberg died. The phenomenon, which was recently covered by Marie Solis at Jezebel, distinctly marks the Trump era; the tweets happened after he was elected, during Brett Kavanaugh’s Supreme Court confirmation hearings, and they’re happening now that President Trump has nominated conservative federal judge Amy Coney Barrettto the Supreme Court.
People who consider themselves pro-choice send a frenzy of posts with one main message: “Go and get an IUD! Our abortion rights are about to be snatched away! We now live in Gilead!”
But this type of reaction falsely implies that everyone in the United States currently has access to affordable reproductive healthcare and that everyone has access to legal and safe abortion care. But, uh, they don’t.
This content is imported from {embed-name}. You may be able to find the same content in another format, or you may be able to find more information, at their web site.
Consider this: If people were relying on an 87-year old woman with pancreatic cancer to stay alive, at least for a couple more months, in order to hold on to the rights afforded by Roe v Wade, what does that say about the state of reproductive rights in the first place?
I’m not trying to discount the seriousness of what President Trump and a Supreme Court packed with his nominees could do. But let’s be real. Your ability to get an abortion depends on your race, class, and zip code, even though, yeah, the practice is technically legal under Roe v Wade. But state laws push abortion access out of reach for poor people and people of color. Abortion rights activists have been sounding the alarm on the damagingconsequencesoftheserestrictions for years.
The crisis isn’t lurking in the shadows, waiting for Barrett to sit on the highest court of the land before it launches an attack. It’s already here.
Just take a look at the way reproductive rights are currently being restricted…
Pro-choice activists outside of the Supreme Court, March 2020.
SAUL LOEBGETTY IMAGES
Public Health Insurance Doesn’t Cover Most Abortion
Passed three years after Roe in 1976, the Hyde Amendment blocks any public health insurance from covering abortion except in life-threatening cases or if the pregnancy is a result of sexual assault. This means that if you get your healthcare through Medicaid, the military, or the federal government, you can’t get abortion care covered, says Sarah Christopherson, Policy Advocacy Director for the National Women’s Health Network. This disproportionately affects poor people and women of color, says Candace Gibson, Associate Director of Government Relations for the National Latina Institute for Reproductive Justice. “In many ways, Hyde was the original abortion ban for many in our communities, making care completely inaccessible to them,” she says.
TRAP Laws Put Unessential Restrictions on Abortion Providers
And obviously, having fewer clinics means that people who need abortions have to travel longer distances and pay more to cover transportation and time off work, making abortion care basically impossible for them.
Outright Abortion Bans Are 100 Percent a Thing
In November, Louisiana citizens will vote on an amendment that would declare there’s no right to abortion in their state’s constitution. West Virginia, Tennessee, and Alabama have already passed similar laws. They don’t immediately impact abortion access, but they could help defend future abortion bans in those states. According to Christopherson, anti-abortion activists passed these Hail Mary laws, even though they know they’ll be challenged, with the hope that they can force courts to rule on laws that chip away at Roe.
Telemedicine Access Is Often Blocked
In 32 states, abortion providers can meet with patients remotely, mail them pills for a medication abortion, and then follow up with them afterwards to see how they’re doing. According to Christopherson, more people are interested in using telemedicine as their preferred abortion method right now because of the pandemic. Some people also prefer the remote option because they don’t have to travel hours to go to a clinic or deal with the harassers outside of them. But right now, access to this abortion method is in danger—the Supreme Court could rule on a case that challenges this soon, and if they say it’s unconstitutional, millions of people will lose access to a safe abortion.
Some States Will Prosecute You for Feticide
Feticide laws are meant to protect pregnant people and their fetuses from assault, but anti-abortion groups use them as a way of giving a fetus the same rights as a human being. As a result, these laws end up criminalizing pregnant people while also disproportionately affecting people of color, according to legal analysesof thesecases. In 2015, Kenlissia Jones, a Black woman, faced charges for delivering a stillborn child after a social worker told police that she had taken medication for an abortion. In 2018, Latice Fisher, a Black woman, was also charged for delivering a stillborn after investigators discovered that she’d searched online for medication for an abortion. And in 2019, Marshae Jones, a Black woman, faced manslaughter charges when she miscarried after being shot in the stomach. This list of women who have been punished for ending their pregnancies could go on and on and on.
Pro Choice Demonstration Outside Dr Emily Women’s Health Center in Bronx, NY, March 2011.
ROBERT NICKELSBERGGETTY IMAGES
So…what do we do now?
If these attacks and restrictions make you feel outraged (hi, same), here are a few things you can do RTFN.
Whether or not Roe is repealed, because abortion access is so patchy nationwide, we need a strong federal standard. Both Christopherson and Gibson mentioned the Women’s Health Protection Act—it’s currently in front of Congress right now, and if passed, it would secure the right to an abortion, no matter what state you live in.
2. SUPPORT GRASSROOTS ORGANIZATIONS—NOT JUST THE BIG SHINY ONES
There are abortion providers, care networks, and abortion funds that fight to bridge the gap between the legal right to an abortion and the actual reality of getting one. Donating to these instead of high-profile women’s healthcare orgs can ensure your $$ does directly to helping people gain access to abortion. The National Network of Abortion Funds has a list of orgs that provide financial aid to help people afford contraception and abortion services—you can donate to the one in your state. The National Abortion Federation and The Abortion Care Network both help to financially support providers across the country.
3. PAY ATTENTION TO LOCAL POLITICS
According to Gibson, “the battle for reproductive justice will not be won in the courts, but in our communities.” This means that we need to pay more attention to the local elections that have a great impact on our lives, not just the presidential one that happens every four years (though, yeah, pay attention to that one, too). Local legislators, judges, and officials have a lot of power to either restrict, or expand, reproductive rights. Read up on the candidates and where they stand on the issues before you head to the ballot box—so you can have a say in WTF is going on no matter who sits on the Supreme Court.


















 Kate at home.
Kate at home.











