Abortion bans throughout Mexico include exceptions for rape. Activists say despite some recent improvements, survivors still confront obstacles to accessing abortion care.

Alma (R) sees her daughter’s ordeal as a form of punishment for their decision to pursue a legal abortion in a conservative region of Mexico.
Meghan Dhaliwal
When Patricia discovered she was pregnant, she tried inducing an abortion with remedies she read about on the Internet: rue tea, aloe, and unsalted bean soup. None of them worked.
Weeks earlier, the 16-year-old was raped by a taxi driver rumored to control the marijuana trade in her neighborhood on the outskirts of Guadalajara, a bustling city in the state of Jalisco, in Mexico’s conservative heartland. Finally Patricia, who asked us not to use her real name, told her mother, Alma. Years earlier, Alma’s mother ignored her daughter’s reports of sexual abuse, and Alma resolved not to make the same mistake. Alma sat her daughter down, and as they talked, Alma took notes. She stressed that whatever happened next was Patricia’s choice, writing “your decision” in a loopy scrawl and circling it. When Patricia said she wanted an abortion, Alma jotted down how they wanted the procedure performed: “Safe—with trained providers. Under the law.” It was January 2016, and Jalisco’s penal code has permitted abortion in cases of rape since 1933. But health department records show that before 2016, no one in the state had obtained a legal abortion under the rape exception.
Patricia and her family live in Tlajomulco de Zúñiga, a poor neighborhood racked by drug-related violence. She was an outgoing teenager who volunteered with the local Green Party, taking classes in urban gardening and helping campaign for the party’s candidates. She loved cooking, and she marveled at how the food reflected her emotions, how her chile de molcajete grew mouthwateringly spicy when she was happy. But after the rape, Patricia withdrew. She was furious one moment, sobbing the next. The smallest sounds startled her. Her rice burned. “I was in shock,” she recalled when we spoke in the fall of 2018, in the studio where her mother works as a beautician. “It was as if my life had been paused and someone had told me, ‘Stay quiet and don’t move.’” She was terrified that if she reported the rape to authorities, her attacker would come after her. But at the time, Jalisco required rape survivors to report the assault in order to obtain authorization from a public prosecutor’s office or a judge for an abortion.
Patricia could have made the 13-hour round-trip journey from their home to Mexico City, where abortion is legal in the first trimester and with no time limit in cases of rape. But that journey can be expensive and logistically complicated, and Alma was a single working mother with other children. Plus, she knew her daughter had the right to abortion in her state. “And if we don’t make those rights worth something, then what are we here for?” she thought.
On January 28, 2016, Patricia and Alma reported the rape to prosecutors, initiating a series of medical and psychological exams, during which they expressed their intention to obtain an abortion for Patricia. None of the officials they encountered gave them a clear answer about how to access an abortion. Finally, on February 10, a psychologist from the attorney general’s office accompanied Alma and Patricia to the state health department. In hand, they had a letter from the prosecutor’s office directing the department to carry out Patricia’s abortion. The following day, they met with the department’s legal director, and on February 12, he called them back to his office. He gave them misoprostol, an ulcer medication that is also used to induce abortions, along with typewritten instructions that read, “one each 8 hours orally; one each 8 hours vaginally” and a phone number for an OB-GYN at the public Hospital General de Occidente. The lawyer gave them the 14-pill foil packet without the box and told them not to tell anyone, not even the prosecutor, according to Patricia and her mother. (In testimony to the Jalisco Human Rights Commission, the legal director denied Alma’s account of these events.)
By the time they returned home, it was dark. The two sat in the living room. “How are we going to do this?” Patricia recalled thinking. “I was very scared, because we didn’t know what would happen.” Around 9 p.m., she took one pill orally and inserted the second into her vagina. By the following morning, she was so weak that she couldn’t walk to the bathroom. It pained her mother to have to continue inserting the pills even as her daughter’s vagina grew inflamed. “I told her, ‘Be patient, mi hija. Be patient,’” Alma recalled. “She was crying, and it was maddening to see her because, apart from her despair, you know that you don’t really know what you’re doing.”
On Sunday morning, nearly 36 hours after Patricia began taking misoprostol, Alma texted the OB-GYN photos of Patricia’s bleeding and concerns about her pain. The OB-GYN agreed to meet them at the hospital, where, according to both women, he abruptly performed a vaginal exam as Patricia wept from the pain. An ultrasound confirmed that she was still pregnant. The instructions the lawyer provided did not match the World Health Organization’s protocol for abortion beyond 12 weeks of pregnancy, which recommends administering the pills every three hours instead of eight. According to Alma and Patricia, the doctor then told Patricia to go home and take more misoprostol, removing the label from the bottle and telling Alma to be careful because, if the police caught them with it, they could be arrested—even though Patricia was seeking a legal abortion from a public hospital. On average from 2007 through 2016 across Mexico, one person was reported to the authorities every day on suspicion of abortion. (The doctor denied this account of the day, testifying to the Jalisco Human Rights Commission that Patricia’s medical care was administered “with quality and warmth and with due information.”)
Patricia began to doubt her decision. “I looked at my mom, and I thought, ‘What am I doing? What is happening?’” she said. “I was resigned to the fact that I was going to have a child.”
Still, the two persisted. Rather than begin a new round of misoprostol, as the OB-GYN suggested, Patricia and her mother met with a lawyer, Angela García Reyes, who told them she would file a legal stay alleging that the state was subjecting Patricia to cruel, degrading, and inhumane treatment by denying her an abortion. The day before that stay was filed, the doctor wrote to Alma saying a judge had authorized the abortion. (According to García, the letter from the public prosecutor’s office should have been sufficient authorization. She speculated that the secretary of health may have been waiting for a judge’s authorization for extra cover in case there was public controversy over the case.) He instructed them to return to the hospital the next morning. But when they arrived, he warned them that the hospital didn’t have “molidas de bebés”—Spanish for “baby grinders,” his term for the equipment necessary to carry out a surgical abortion. Instead, Patricia would be administered more medication to end the pregnancy.
The following morning, Patricia was admitted for what staff members described as their first abortion case. (State records show there was one abortion in the month before hers in the same hospital, but local lawyers and activists said they have no memory of such a case.) The medical staff placed her in a bed in a corner of the maternity ward echoing with the sound of women in labor, and they barred her mother from entering the room. At one point, Patricia recalled a gaggle of about 15 medical students clustering around her. She was told to open her legs, and someone painfully inserted a speculum. According to medical records, the medical staff administered mifepristone and misoprostol with the aim of inducing labor. She said the doctors subjected her to more than a dozen vaginal exams. Nurses drifted by her bed, chiding her, “You do know that the babies aren’t to blame?” Hours later, she was injected with oxytocin, a hormone used to induce labor, and her contractions grew so painful that she cried out for help. A medical worker moved to inject her with a pain medication, but a doctor intervened. “We’re not going to give you anything for the pain,” Patricia remembered her saying. (According to the medical records, during this phase of the abortion, Patricia was given an anti-inflammatory medicine known as keterolac, which has some analgesic properties, and another medicine used to treat cramping. The hospital did not respond to requests for comment.) Finally, more than 12 hours after she was admitted, Patricia felt a sensation similar to defecating, and the room grew blurry. She was wheeled into the surgical ward. Doctors performed a curettage to remove the remains of the pregnancy.
It had been 22 days since Patricia first reported the rape. Alma sees her daughter’s ordeal as a form of punishment for their decision to pursue a legal abortion in a conservative region of Mexico. “It was like they were telling her, ‘You chose this, right? Well, then this is what’s going to happen.’”
* * *
In Mexico’s groundbreaking national elections in 2000, the right-wing Partido Acción Nacional (PAN) ousted the Partido Revolucionario Institucional (PRI), at the time the longest-ruling party in the world. Abortion rights activists feared that members of the conservative government would seek to further restrict abortion in Mexico, which at the time was legal only for rape survivors and, in some states, in other instances, such as if the pregnant person’s life was in danger or for serious fetal anomalies. Indeed, the month after the elections, lawmakers in the president-elect’s home state of Guanajuato moved to ban abortion in cases of rape in that state. The effort sparked such massive street protests that the state’s interim governor was forced to veto the measure. Although the law failed, abortion was nearly impossible for rape survivors to obtain. According to a 2006 Human Rights Watch report, “actual access to safe abortion procedures is made virtually impossible by a maze of administrative hurdles as well as—most pointedly—by official negligence and obstruction.” In Jalisco, one social worker boasted to Human Rights Watch about having persuaded a child who had been raped by her brother not to end the pregnancy, saying, “She came here wanting to have an abortion, but we worked with her psychologically, and in the end she kept her baby. Her little child-sibling.”
Mexican feminists scored an extraordinary victory in 2007, when Mexico City legalized all abortions in the first trimester. But in the ensuing years, more than half of Mexico’s states passed constitutional amendments to define life as beginning at conception, joining Chihuahua, which reformed its Constitution in 1994. While not enforceable, these measures contributed to a sense of uncertainty around access to legal abortion. Meanwhile, the U.S.-backed drug war, which began in 2006, fueled soaring levels of violence across the country, including rape and femicide. Women activists and victims’ families mobilized to bring attention to this crisis and demand protections, including abortion access for rape survivors. In 2012, with more than 100,000 people killed and 25,000 more disappeared in the previous six years, lawmakers passed a General Law of Victims. Among other things, it affirmed the right of rape survivors to access legal abortions in public hospitals. Advocates then successfully pushed federal authorities to reform a rule, known as Norm 046, to say that rape survivors could obtain an abortion without authorization from a judge or other authority and that those age 12 or older could do so without a parent’s permission. The reform took effect in 2016—a month after Patricia had her abortion—and the Supreme Court upheld it this August. The same year, activists pressured Jalisco to declare an alert over gender violence, activating a legal mechanism that feminists have used to push authorities to improve access to abortion in cases of rape.
Despite these reforms, in prosecutors’ offices and public hospitals across the country, procedural barriers remain deeply entrenched. In a report tracking cases from 2012, the year before the General Law of Victims took effect, to 2018, two years after the reform of Norm 046, the reproductive rights organization Grupo de Información en Reproducción Elegida (GIRE) said it supported 38 rape survivors, the majority of whom were under 18, who were denied abortions or faced serious hurdles. In 2015 in Tabasco, the public prosecutor’s office attempted to reclassify a 10-year-old’s rape as pedophilia in order to disqualify her from accessing an abortion. (She ultimately obtained the procedure.) In 2016 an 18-year-old farmworker was denied an abortion in Baja California Sur because, according to local authorities, “abortion is a crime because it is an attack against a child.” In 2018 a 15-year-old reported to authorities in Puebla that she had been raped by her uncle and needed an abortion, but local authorities told her that abortion there was illegal, making her fear that she would be arrested for obtaining one. She and the farmworker had their abortions in Mexico City.
Before the General Law of Victims took effect, one woman was even imprisoned. In 2012 a 26-year-old in Durango obtained an abortion after being kidnapped, raped, and impregnated by her ex-boyfriend, who later threatened to kill her unless she dropped the charges against him. When she complied with his demands, local authorities charged her with making false statements and the crime of having an abortion. She went to prison.
Data collected by GIRE suggests that, despite the prevalence of sexual violence in Mexico, few abortions have been provided in cases of rape, even in the years since the reforms. GIRE found that from December 2012 to October 2017, public health-care institutions reported performing 137 abortions in cases of rape, an average of 27 each year nationwide, even though thousands of rapes are reported each year.
* * *
Mexican activists credit survivors like Patricia, who have asserted their legal rights within a hostile system, with spurring limited improvements in recent years. “It was these women, these girls, who came forward and said, ‘Yes, I’m going to do it,’” said Verónica Marín, an activist who helps rape survivors in Jalisco. “We accompanied them, but it was their bodies that endured that torment.”
For more than a decade, Marín and other activists have supported women and girls in Jalisco who traveled to Mexico City to end their pregnancies. From 2009 to 2016, when there were 111,413 rapes reported to federal and local attorneys general, public health authorities reported performing only 63 abortions in cases of rape. About two-thirds of these were reported by Mexico City. According to government statistics, just over 600 people from Jalisco have traveled to Mexico City for legal abortions over the last 12 years. Countless more have chosen to self-induce using misoprostol pills, which are available in street markets and over the counter in pharmacies. Grassroots feminist groups have sprung up across Mexico to help people safely take this medication. Self-managed abortion is legal in cases of rape, but rape victims who pursue that option and experience complications that require follow-up care risk being reported to authorities if providers don’t believe they were raped. Government records show that nationwide, authorities prosecuted 157 women for having an abortion from 2014 to 2017. In Jalisco illegal abortion carries a sentence of up to two years in prison, and other states impose sentences of up to six years for patients and 10 years for providers. Women who self-induce abortion, or suffer miscarriages or stillbirths, have faced murder and infanticide charges. People in rural areas, including indigenous women, may lack access to safe methods of abortion and are more likely to resort to dangerous methods. Unsafe abortion is a leading cause of maternal death in Mexico.

Activists Verónica Marín (L) and Patricia Ortega (R)
(Amy Littlefield and Laura Gottesdiener)
Several years before Patricia’s case, Marín and other activists began helping rape survivors demand that public hospitals provide abortions. They wanted to force the hospitals and the Mexican state to make good on their legal rights, but they also wanted to pave the way for decriminalizing abortion by compelling doctors, who are authority figures in Mexican society, to perform the procedure. Marín said that having doctors provide abortion in public hospitals, as opposed to women secretly taking pills at home, would help destigmatize the procedure. “It has to be in the health centers. It has to be done via the state,” said Marín, a vibrant woman with blue-streaked hair, “because if the state is doing it, then how can the state criminalize it?”
When Marín and others started trying to help rape victims access abortions in Jalisco, there was no clear protocol, and the authorities simply refused. Time after time, the activists helped victims travel to Mexico City. Even after some public hospitals began to perform the procedure around the time of Patricia’s case, Marín said, hospital authorities continued to treat both patients and activists with hostility. Sometimes staffers called security to oust the activists. When providers failed to give victims pain medications, the advocates would smuggle pills to them hidden inside their clothing. “When we began,” Marín said, “it seemed impossible that one day a hospital would practice abortions and that the whole world would know it was happening there.”
* * *
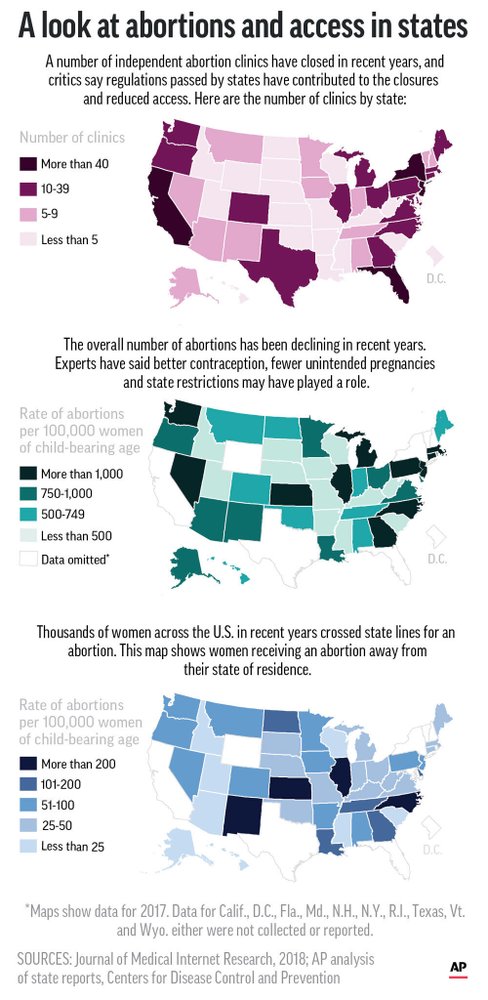
Today, though the national law says rape survivors in any Mexican state can go to a public hospital and get an abortion without reporting the crime to authorities first, 11 states still have laws on the books that require victims to file a report. The national law nullifies such requirements, but “the lack of compliance of some penal codes with the national legislation concerning care of victims disadvantages women in certain states, who face higher barriers to access abortion services depending on their geographic location,” GIRE concluded last year. Twelve states impose some form of time limit on abortion for rape survivors, mostly confining it to the first trimester of pregnancy. The patchwork of state-level abortion laws in Mexico parallels that of the United States, where access also depends largely on a person’s location and ability to afford to travel to the nearest clinic. Interest in self-induced abortion has spiked in the United States after the confirmation of two U.S. Supreme Court justices nominated by President Donald Trump, which has raised the prospect that the Court will overturn Roe v. Wade and allow some states to ban abortion outright. Some emboldened Republicans have dropped rape exceptions from their increasingly extreme efforts to ban the procedure. But many, including Trump, still support these exceptions as a way to temper opposition among an American public that overwhelmingly supports abortion access for rape survivors. In Mexico, such exceptions have yet to fulfill their promise of protecting these victims.
Since Patricia’s case in 2016, public hospitals in Jalisco have performed at least 20 abortions for rape survivors, according to records provided by officials in October 2018. Otilia Bibiana Domínguez Barbosa, the coordinator of the gender-based-violence program at the Jalisco Health Department, said in an interview that since Patricia’s case, the state has implemented a protocol for rape survivors and is conducting trainings for providers.
García, the attorney who represented Patricia, said she has seen improvements in the legal system in Jalisco but not as much among health-care providers. “I think that the laws, the judges are slowly understanding that this is a right that we have as women. But the health sector is still behind. The health sector is the barrier we are pushing up against,” she observed. Across the country, activists said that one of the biggest remaining hurdles is not the law itself but rather the doctors, nurses, hospital administrators, and other public officials who fail to understand it or refuse to carry it out.
Many of these providers claim a religious opposition to abortion. In an interview last October, Domínguez said she knew of only 28 doctors in the entire state who were not registered as conscientious objectors to abortion—up from nine the year before. This year, a young rape victim was forced to file a lawsuit after authorities in the state of Aguascalientes denied her a legal abortion, claiming that there were no people who were not conscientious objectors available to carry out the procedure. (A federal judge then ordered Aguascalientes to provide her an abortion within ten days.) “We have a beautiful legal framework in Mexico,” said Esmeralda Lecxiur Ferreira, a legal adviser with the reproductive health services group Mexfam. “The problem is that the authorities are not interested in implementing it.”
Indeed, in two cases in 2017 and 2018, rape survivors continued to confront obstacles to accessing legal abortion in Jalisco—including at the same hospital where Patricia went. In September 2017 a 16-year-old named Juana (who asked to use a pseudonym) sought a legal abortion after being raped by two men while she was walking to school in her rural town in the interior of Jalisco. She and her father traveled hours to Guadalajara to obtain the procedure. But from the moment they arrived at the hospital, Juana said, she felt that the doctors didn’t want to take care of her. According to Yazmín Cano, an activist who accompanied Juana, the doctor in charge of the legal abortion program initially refused to treat her because she didn’t have documents showing she reported the crime to authorities, even though the reform of Norm 046 made it clear that rape survivors could obtain an abortion without authorization. Cano said the doctor then tried to intimidate Juana, warning that the abortion could perforate her uterus, leaving her infertile or even killing her. (The hospital did not respond to requests for comment.) After insisting that she wanted an abortion, Juana was given medication and, like Patricia, found herself sequestered in the labor and delivery room. “They left me pretty much alone, dying of pain,” she recalled. “To this day, I close my eyes, and I still see the women who were giving birth. It was very traumatic.”
The activists got observers from the state’s human rights commission to go and witness Juana’s treatment. Finally, Cano said, the doctors ended her pregnancy surgically. “I think that the doctors didn’t want to participate in the curettage because for them and for many people, this is a crime—abortion is a crime,” Juana said. The next morning, as she was recovering from the surgery, a police officer arrived and interrogated her and her father separately about the rape, even though she had not reported it. She said she felt her rights were violated in the hospital but, despite the trauma, she doesn’t regret seeking an abortion. She’s now attending nursing school and is passionate about her studies. “Even though the whole world criticizes you, you have to keep living, for yourself most of all,” she said.
A year after Juana’s case, García accompanied a rape victim to another public hospital in Guadalajara, where the staff had undergone training by an abortion rights organization. The victim didn’t face any legal barriers, but according to García, the hospital prevented the patient from meeting with her and called the patient’s family to disclose the rape and the abortion, even though García had expressly told the hospital that the patient didn’t want her family to know and the law allows victims age 12 or older to get an abortion without a parent’s permission. “It’s a daily, daily, daily fight with the health-care institutions,” García said.
Recent Supreme Court rulings in favor of rape survivors’ accessing abortion have given legal advocates more ammunition. The rulings granted damages to victims and ordered improvements by health-care authorities. “We as civil-society organizations are disseminating the information and saying to the hospital authorities, ‘Look, you can be held responsible for denying services,’” said Fernanda Díaz de León, a senior policy adviser at Ipas, an international reproductive health organization. Still, the rulings don’t subject individual providers to penalties.
Another issue is the lack of education among not just officials but also the public, including rape survivors themselves. Patricia Ortega, a Jalisco activist who works with Marín, said that before 2016, though the rape exception was in the penal code, no one—including the most sympathetic public officials—knew how to make it a reality. “Now there is a clear procedure, and when victims have that information, they can arrive [at the hospital] and argue this is in the official norm,” Ortega said. “What is lacking now is public awareness.”
Many people still think that abortion is a crime in all cases, she added—leading GIRE to conclude that “while abortion is considered a crime instead of a health-care service, women will keep confronting violations of their reproductive rights, including when they seek abortions under circumstances allowed by law.”
* * *

Activists on International Safe Abortion Day in 2018
(Amy Littlefield and Laura Gottesdiener)
Many advocates say that justice for rape survivors will not be fully realized in Mexico until abortion is both decriminalized and more widely accepted within the country’s conservative culture. Two years after Patricia fought to obtain her legal abortion, a “green tide” of pro-choice activism began to sweep across Latin America, with hundreds of thousands of people pouring into the streets to demand the legalization of abortion across the region. Countries in Latin America and the Caribbean have some of the world’s most restrictive abortion laws, with several banning abortion outright. A few allow it without a specific reason in the first trimester, and the rest ban it with various exceptions, including to save the pregnant person’s life or in cases of rape. In 2014 at least 10 percent of maternal deaths in the region resulted from unsafe abortion, according to the Guttmacher Institute, a reproductive health research organization. The green tide began in Argentina, where a grassroots feminist movement brought a million people to the streets to support a historic vote to legalize abortion. Although the bill they supported ultimately failed, the effort galvanized the abortion rights movement across the region.
Mexican activists have been emboldened. “When we saw everything that happened in Argentina, that gave us a breath of fresh air and renewed our energies here in Mexico,” said Daniela Zaizar, a 24-year-old activist. Pressured by the green tide, members of the left-wing Morena party of Mexican President Andrés Manuel López Obrador have sent some hopeful signals. Interior Minister Olga Sánchez Cordero has said she supports decriminalizing abortion up to 12 weeks and releasing all women currently incarcerated for abortion-related crimes.
On September 28, thousands of people are expected to fill the streets of cities across Mexico for the annual International Safe Abortion Day. Last year, hundreds of women wearing green handkerchiefs and T-shirts poured into the streets of Guadalajara to demand the decriminalization and acceptance of a procedure undergone by countless women in Mexico. Some of the protesters said they were inspired to march after their experiences with extralegal abortions. Patricia said she hoped to attend the march, but it was too far from home for her to travel alone, and her mother was at work. Instead, she shared information about the event on social media. Posting publicly about the march made her nervous, given how critical she knew people could be about abortion. But she decided to do it anyway. Much to her surprise, some of her friends liked her post. One male friend who worked in a public hospital replied simply, “I support you.”
Source: https://rewire.news/article/2019/09/17/mexico-abortion-exception-rape-survivors/
Share what you read here: