Students participate in a Teen Talk High School class in Belmont, Calif. Sex education in some American high schools is evolving beyond pregnancy and disease prevention to include lessons aimed at curbing sexual assaults.JEFF CHIU/AP
Amonth ago, the federal government sent a “Dear John” letter to the Children’s Hospital Los Angeles.
“Due to changes in program priorities,” the letter began, “it has been determined that it is in the best interest of the Federal government to no longer continue funding” the grant for one of our hospital’s teen pregnancy prevention programs. This one-page form letter, sent from the Department of Health and Human Services, arrived almost a year to the day that HHS initially approved our five-year project with glowing reviews about how the Children’s Hospital Los Angeles is “recognized for innovative service and training models, leadership in community collaboration, and research regarding adolescent issues” and has “over 50 years of experience in implementing programs in safe and supportive environments for youth and their families.”
This teen pregnancy prevention program, which we oversee, wasn’t the only one to be abruptly dumped. The Trump administration withdrew nearly $214 millionfrom 80 HHS-funded teen pregnancy prevention programs across the country. The HHS didn’t give us a reason for the decision.
So far, the only explanation we’ve been able to glean is an HHS statement to the Associated Press reportedly saying that only four of 37 programs they evaluated had shown evidence of lasting positive impacts, while the other 33 programs had no effect or were harmful.
To this day, we don’t know, nor do our colleagues in the teen pregnancy prevention community, exactly why these cuts were made. Not even our U.S. senators seem to know.
As an organization that has been involved in developing, implementing, and evaluating teen pregnancy prevention programming for more than 30 years, Children’s Hospital Los Angeles is deeply concerned about the long-term effects these cuts will have on teen birth rates and on the lives and health of young people around the country.
Before we go on, let us be clear: Teen pregnancy is still a problem in the United States. Our country has the highest teen birth rate — 57 per 1,000 females ages 15 to 19 — among 20 countries with complete birth statistics. In 2015, 230,000 babieswere born to women ages 15 to 19. And less than 5 percent of sexually active teens use the most effective forms of birth control.
That said, the teen birth rate in the U.S. has been dropping, and hit an all-time low in June 2017. The Centers for Disease Control and Prevention and the American Congress of Obstetricians and Gynecologists credit evidence-based teen pregnancy prevention programs with this dramatic decline.
So we’re confused by claims that these programs aren’t working. And we don’t understand why the administration is choosing to bulldoze them just as we are getting a handle on the issue.
It’s possible that our country’s successes in curbing teen pregnancy have led some to believe that such cuts will allow us to save money on a problem that has already been solved. That couldn’t be further from the truth.
The funding that Children’s Hospital Los Angeles lost would have helped us train and work with other HHS grantees to ensure that their teen pregnancy prevention programs continue to adapt and respond to new challenges, like reaching populations often neglected in the past like LGBT youth; being more responsive to the needs of youth who have experienced past trauma; and promoting more authentic youth-adult partnerships where young people are actively involved and not just passive consumers of information.
Unlike the sex education programs that many of us endured between the 1950s and the 1990s, those funded by HHS in the last decade have been more targeted and more accountable than ever. They focus on delivering medically accurate and comprehensive sex education, and require that grantees use interventions and methods proven to be effective. Today’s programs include multiple sessions; interactive and engaging curricula; and focus on life skills like decision-making, communication, and goal-setting.
The HHS decision to de-fund these programs:
takes a big step away from evidence-based interventions
will slow or stop the momentum needed to reduce early and unplanned teen pregnancies
represents a significant disinvestment in the lives and health of adolescents nationally, particularly those living in poverty and in under-resourced communities.
For young women and young men, early childbearing is significantly linked with dropping out of school. That means teen pregnancy prevention programs do more than just prevent youths from becoming parents. These programs prevent poverty and teach youth the core skills needed to make healthy choices. In essence, they help create successful adults.
“It seems as if the documented frequency of miscarriages or fetal demise is forgotten and the immediate thought is foul play.”279
At a hearing on August 7, Skylar Richardson pleaded not guilty to the charges and Fornshell asked for a million-dollar bond “due to the severity of the crime.”
Sonia Chopra
Texas has seen some of the nation’s most regressive abortion restrictions in recent years. This series chronicles the fall-out of those laws, and the litigation that has followed.
A trial date has been set in the case of Brooke Skylar Richardson, the 18-year-old Ohio woman who has been accused of killing her baby after telling her doctors she’d given birth to a stillborn child.
Richardson was recently indicted on five counts including aggravated murder, involuntary manslaughter, child endangerment, tampering with evidence, and gross abuse of a corpse. These charges stem from the discovery of skeletal remains found in the backyard of the Carlisle home where Richardson has lived with her parents for her entire life.
The investigation began July 14, after the police received a call from a doctor at the Hilltop OB-GYN clinic saying that Richardson had reported a stillbirth. Hours later, investigators showed up at the home of Richardson’s parents, Michael and Kimberley, with a search warrant and found the remains. Police said an autopsy later revealed a live birth, though they have not been forthcoming about what evidence was used to support this.
After Richardson was initially arrested on charges of reckless homicide, the family cooperated with investigators and sat down to interrogations over a two-day period without an attorney present. Warren County Prosecutor David Fornshell then presented the case against Richardson to a grand jury, which indicted her on the five counts.
At a hearing on August 7, Richardson pleaded not guilty to the charges and Fornshell asked for a million-dollar bond “due to the severity of the crime.” Judge Donald Oda II set bond at $50,000, saying that he did not believe she poses an “imminent threat” to the community and that he has seen little evidence for the serious accusations.
After Richardson posted bond, she was fitted with an ankle monitor and put on house arrest. Her trial will begin November 6, with the next hearing scheduled for August 25.
Between the time of the first arrest and the formal accusation, Fornshell and investigators were tight-lipped and refused to make any statements apart from holding a press conference August 4, at which Fornshell accused Richardson of giving birth before burning the body and burying it in the backyard.
“I am not sure we ever will provide to you the exact medical cause of death and the reason for that is because the child was, after death, burned and subsequently buried and there was significant decomposition to the body,” Fornshell said at the conference. Based on the bone measurements, Fornshell said, Richardson had been 38 to 40 weeks pregnant.
Fornshell added that he has decided not to seek the death penalty, but he is pursuing the murder charge as a special felony and is seeking life in prison for Richardson, if she is convicted.
A few days after Richardson’s August 7 hearing, Fornshell posted on social media that “testing has confirmed the baby was born a girl.” That same day, news emerged that Judge Oda had issued a gag order for all parties in the case. He identified 13 links from published media reports in his motion and said he wanted to ensure a fair trial.
Before the gag order, Richardson’s attorney Charlie M. Rittgers told Rewire that he has, so far, seen no evidence to support the prosecution’s accusations. Although he does not have discovery—the ability to obtain evidence from the prosecution—he intends to seek the assistance of independent experts to examine the remains.
Rittgers said that Richardson, who goes by her middle name, Skylar, has “led an exemplary life” so far.
“She is a good person. A good student who has been a high honors student all her life. She has never been in any trouble of any kind. She was every teacher’s pet,” Rittgers said, pointing out that Richardson had been a cheerleader and on the student council for three years. Richardson just graduated from Carlisle High School and was planning to go to the University of Cincinnati in the fall. In the past, Rittgers said, she had participated in a youth retreat program and volunteered with Bogg Ministries, where she served meals to homeless people. According to her attorney, she has also helped children with disabilities learn cheerleading through a local nonprofit.
Her high school and the YMCA where she worked at the time of her arrest have declined comment to all media requests.
“She didn’t drink. She wasn’t a partier or a smoker. By all measures, she is a good girl who helped children …. She is a good person,” Rittgers said. “This is a tragic situation and Skylar is taking it in the way you would expect: It has shocked her.”
Richardson’s peers and neighbors, who spoke about her and her family on condition of anonymity, told Rewire that she was a “serious, quiet girl” who hung out with very few kids and never “bothered anyone at school.”
Richardson’s case has also attracted national attention from advocates who note that it bears some resemblance to that of Purvi Patel’s, the Indiana woman who was arrested after prosecutors said she delivered a live fetus following taking abortion-inducing drugs obtained from the internet. Patel was ordered to serve 20 years in prison for feticide and felony neglect of a dependent in 2016. After an appeal, the feticide charge was overturned and the neglect charge was reduced last year.
“Reading about the Richardson case brought a sense of dread and déjà vu,” said the Rev. Marie Siroky, a board-certified chaplain and ordained minister in the United Church of Christ in Indiana. Siroky has spent much of her life as an advocate who ministers to women who are prosecuted after the outcome of their pregnancies.
“The prosecutor states it was a live birth while saying that the cause of death may never be known due to the conditions of the remains. Where is the evidence of live birth?” she asked.
Referencing Patel’s case, Siroky said, “I want to make it very clear that I do not condone that [corpses] be buried or thrown into dumpsters, but who knows what is happening to them at that moment. It’s easy to judge after the fact.”
Siroky is distressed at Fornshell’s speculation into Richardson’s motive: that she “purposefully caused the death of the child” to maintain her “good girl” appearances. At the press conference, Fornshell said that he is “pro-life” and this case “affects him as a father” because his daughter is at the cusp of the teen years.
As a chaplain, it upsets Siroky that health-care providers alert police with no evidence of a crime. “It seems as if the documented frequency of miscarriages or fetal demise is forgotten and the immediate thought is foul play,” Siroky said. Although miscarriage frequency is difficult to pinpoint because individuals may not realize they are pregnant, studies show that anywhere from 10 percent to 25 percent of all clinically recognized pregnancies will end in miscarriage.
Nancy Rosenbloom, director of legal advocacy at the National Advocates for Pregnant Women in New York says that she has worked on similar cases nationwide where the prosecutors punish women who give birth under what they consider “suspicious circumstances.”
“To prosecute women for a pregnancy loss is not a good policy, but the authorities act on it as if it is a basic principle. [Women] have a right to seek medical treatment without the prospect of prison hanging over their heads,” Rosenbloom said.
Rosenbloom says that while “we don’t know what happened,” with Richardson, she believes that the “case will require a lot of actual evidence” to prove the prosecution’s theory. She notes many tests like the “lung float test” that prosecutors might use to prove that a baby drew a single breath are faulty and widely discredited.
Some who agree with the prosecutor’s conclusions point to the age of the teen, saying his proposed sentence is too strong.
“I’m sad for this young woman and think that the prospect of life in jail is too harsh,” said the Rev. Rebecca J. Tollefson, executive director of Ohio Council of Churches, in an interview with Rewire.
“I understand that there needs to be justice as well. Maybe she needs to enter a program for respecting herself and accept the consequences of her decision. The greater question is how can the law assist [her] to be a better person,” Tollefson said.
Since news first emerged about Richardson’s case, social media has been set ablaze with comments about the young woman, with some calling her names such as “child killer” or “baby killer.”
Two protesters showed up at the recent court hearing and confronted the Richardson family. Cherie Young and Karen Miller said they were the voice of “Baby Carlisle” and they held signs that said, “Abortion is legal, Murder is not.” The Richardson family did not acknowledge the pair.
While local attorneys and judges have declined to comment on the case, Judge Norbert Nadel, a retired judge from nearby Hamilton County has been unable to resist the temptation to add his opinion, telling WCPO Channel 9 (and repeating to Rewire) that Richardson’s bail was set far too low.
Many caution that the presumption of guilt is unhelpful and will hamper the chances for a fair trial. Siroky, for example, noted that existing media coverage did not do the case justice. “Thankfully, the judge has imposed a gag order. However, the damage is done. While the quote that Richardson killed her baby is attributed to authorities, the evidence behind the quote is missing,” Siroky said.
“People are premature in their judgments. Most of the facts of the case have yet to be released and frankly, they are still unknown to me,” Rittgers said.
“I want people to have an open mind and withhold their judgments until we get discovery,” he continued.
“There was nothing in The Heidi Group’s operations or history to indicate that this non-medical organization was even remotely qualified to provide comprehensive reproductive healthcare.”
Carol Everett, the group’s CEO, placed most of the blame for the organization’s subpar performance on the clinics with which it works. FacingLifeHeadOn / YouTube
Evidence provided to Congress by state attorneys general and health departments proves that abortion is both extremely safe and highly regulated. Searchable by state.
A Texas anti-choice organization contracted to distribute millions in state funds for family planning services has failed to provide the services promised. State officials responded by slashing the organization’s funding.
The Heidi Group was awarded $1.6 million in August 2016 to provide services through the Healthy Texas Women Program, along with a contract to distribute $5 million to a network of family planning providers serving Texans with low incomes.
Carrie Williams, a spokesperson for the Texas Health and Human Services Commission, told the Associated Press that the Heidi Group will now receive less than $1 million for family planning services.
“They didn’t reach their own targets during this first year of ramp up,” Williams told the AP. “We’re adjusting the amounts to make sure we are maximizing services for women through our contractors.”
Heather Busby, executive director at NARAL Pro-Choice Texas, told Rewire in an email that the Heidi Group contract was an example of Texas officials placing “politics over people.”
“There was nothing in the Heidi Group’s operations or history to indicate that this non-medical organization was even remotely qualified to provide comprehensive reproductive health care,” Busby said.
Carol Everett, the Heidi Group’s founder and CEO, set ambitious expectations for the organization when it submitted a bid for the state contract. The Heidi Group’s application listed 16 subcontractors operating 20 clinics. The organization projected that it would provide family planning services to more than 50,000 clients.
But Everett has reportedly struggled with outreach efforts as the group’s network of providers has failed to meet more modest goals. Williams told the Associated Press that the organization now plans to serve only a “fifth of the nearly 18,000 women originally projected.”
Everett has placed most of the blame for the organization’s performance on the providers, but it remains unclear how many providers remain in the organization’s network and how many clients they are serving.
Connie Wyatt, CEO of Wise Choices Pregnancy Resource Center, told Rewire in a March email that she attended a “roll-out meeting” for the program in August 2016 but decided not to be part of the program.
“When the program was rolled out, it did not come through as the lawmakers originally stated it would, and therefore, we did not finalize as a subcontractor with Heidi Group nor did we participate in the program or ever apply for or receive funds,” Wyatt said.
Busby said the state’s decision to “award undeserved millions of taxpayer dollars” to the Heidi Group was driven by ideological opposition to Planned Parenthood. “Tens of thousands of Texas in need of health care will pay the price for our state leadership’s unhealthy relationship with anti-abortion zealots like Everett,” Busby said.
A policy offering free terminations for those who can travel is a first step. Now we need to change the law for those who can’t
‘Until now women in Northern Ireland have had to take their chances in organising their own terminations at clinics that are not equipped to deal with serious medical conditions.’ Photograph: Charles McQuillan/Getty Images
Northern Ireland’s Department of Health has declined to issue new guidance on abortion to doctors and other health professionals because “there has been no change to the law on abortion”. This is despite the fact that the situation clearly has changed since women from the region can now access free, NHS abortions in England.
This stubborn refusal to recognise the reality of women’s reproductive healthcare needs is concerning because it ignores the fact that, at present, GPs in Northern Ireland are not permitted to purchase procedures outside Northern Ireland “that would be illegal in Northern Ireland”. This prohibition clearly needs to be updated to take account of the new situation.
Since the end of June, women from Northern Ireland can receive free NHS abortions through self-referral to the British Pregnancy Advisory Service or Marie Stopes; these agencies will then recoup the costs from the Equalities Office. Leaving aside the cost, financial and emotional, of having to travel for healthcare, this should work well for women who need an abortion mainly because they do not want to be pregnant.
But a small minority of women need, for medical reasons, to have their terminations in a hospital setting. With only 16 abortions carried out in Northern Ireland by health professionals in 2014-15 and again in 2015-16, clearly women with a range of health issues are not able to access legal abortions in Northern Ireland. Until now, they have had to take their chances in organising their own terminations at clinics that are not equipped to deal with serious medical conditions.
If nothing else, GPs need to be informed of care pathways through which these women can end their pregnancies in hospitals where all their medical needs can be met. It was to help such women that the idea of NHS-funded abortions for women from Northern Ireland first arose.
After the 1997 general election, hopes were high that the 1967 Abortion Act would be extended to Northern Ireland, particularly since both Tony Blair and Mo Mowlam, then secretary of state for Northern Ireland, had voted while in opposition for the extension of the act. However, it soon became clear that women’s rights were to be sacrificed to the “peace process”. Mowlam later admitted she “would have liked to have done something” for women in Northern Ireland but could not – for fear of “stirring up the tribal elders”.
Together with Voice for Choice, campaigners in Northern Ireland began to look at free NHS abortions as a stopgap measure that would reduce the inequality of access a little.
In February 1999, Maria Fyfe, then Labour MP for Glasgow Maryhill, wrote to Mowlam about abortion law in Northern Ireland. Adam Ingram, then a minister of state in the Northern Ireland Office, replied on Mowlam’s behalf on 10 March 1999. He wrote: “You raised the possibility of arrangements being introduced to enable GP fundholders and their purchasing authorities in Northern Ireland to fund terminations of pregnancy carried out elsewhere in the United Kingdom. I understand that such arrangements would not be possible in the case of fundholders who … are specifically prohibited from purchasing treatment for their patients outside Northern Ireland which would be illegal in Northern Ireland, such as termination of pregnancy.” (Of course, termination of pregnancy is the only treatment available in the NHS which would be illegal in Northern Ireland.)
The Northern Ireland assembly has shown itself incapable of dealing with the reality of abortion in the region. Debates have tended to be high on anti-abortion rhetoric and low on practical approaches to the reality of women’s lives in the 21st century. For almost 20 years now, Westminster has looked the other way. Indeed, a letter sent at the end of June from Justine Greening, the minister for women and equalities, to MPs – setting out the government’s proposal to provide NHS abortions to women from Northern Ireland – ended with an assurance that “none of this changes the fundamental position that this is a devolved issue in Northern Ireland … This announcement does not change that position”.
Women in Northern Ireland continue to be discriminated against. Westminster cannot devolve human rights; it remains the guarantor of such rights despite devolution. The (non-)response of the Northern Ireland Department of Health to the changed situation reinforces the view that Stormont is incapable of bringing women’s rights into the modern era and ensuring full reproductive healthcare in local hospitals.
The move to give everyone access to NHS abortions in Britain is a step in the right direction, but it is only the first step. Now Westminster needs to act to end half a century of inequality for women in Northern Ireland.
After the election, a new “back to the basics” approach at Planned Parenthood made organizing a priority during the months-long health care debate. The next project: recruiting and training hundreds of volunteers spread out around the country.
Joe Raedle / Getty Images
Planned Parenthood canvassers go door to door about the Zika virus in Florida last month.
Planned Parenthood wants to put the next health care fight in the hands of its volunteers.
Over the next 12 months, the 100-year-old women’s health and abortion rights group will build a corps of 600 volunteer-led community organizing teams across the country, each one located near a Planned Parenthood health center, officials said this week.
The new organizing project, seeded with an initial $500,000, begins in September with four regional “bootcamps,” where 1,000 hand-picked volunteers will undergo intensive training, return home with new organizing tools, and form the basis of an effort that Planned Parenthood officials believe is “unlike any other than we’ve ever made.”
That’s how Planned Parenthood’s national organizing director Kelley Robinson described the decision to invest in a nationwide network led entirely by volunteers, focused on building “intersectional” local campaigns to “protect and promote” women’s health. (The $500,000 will be a joint investment made by the Planned Parenthood Federation of America and its linked political arm, Planned Parenthood Action Fund.)
For the volunteer leaders that Planned Parenthood trains next month, that could mean building local campaigns around legislation in Washington, or sexual-assault awareness on campuses, or ballot initiatives in the state. The idea more broadly, said Nilofar Ganjaie, a lead Planned Parenthood field organizer based in Seattle, is “to actually put this the hands of activists” and “scale up in a way that we haven’t been able to do.”
Looking ahead after the Republican health care defeat, officials see that kind of self-organizing network as the key to more “long-term power” — and the next step in a recommitment to grassroots organizing at Planned Parenthood first set off by last year’s election.
The organization spent millions to support Hillary Clinton’s campaign, including a $30 million push targeting millennial voters in the final stretch to Election Day. When they lost, said Robinson, “the strategy for our organization was called into question.”
“It was time for us to start going back to our block and tackle, meaning it was time to go back to the basics — the things that we’ve always done well to survive in the last 100 years,” she said. “We started thinking about our grassroots first.”
Over the next nine months, as Republicans worked to repeal the Affordable Care Act, and cut or redirect federal funding for Planned Parenthood, the organization developed new organizing tools and added 226,000 volunteers and 1 million total supporters.
In the lead-up to last month’s vote, they held 2,400 marches, meet-ups, phone banks, and rallies, and collected 1 million petition signatures, according to the group. They made 200,000 phone calls to members of Congress, followed by calls to people who live in the same state to tell them to call their members of Congress (including 20,299 to tell Nevadans to call Sen. Dean Heller). They drafted 90,000 supporters to a “Defenders” program, with tools for “real-world actions” and an “Emergency Guide” to the latest “urgent action to focus on.”
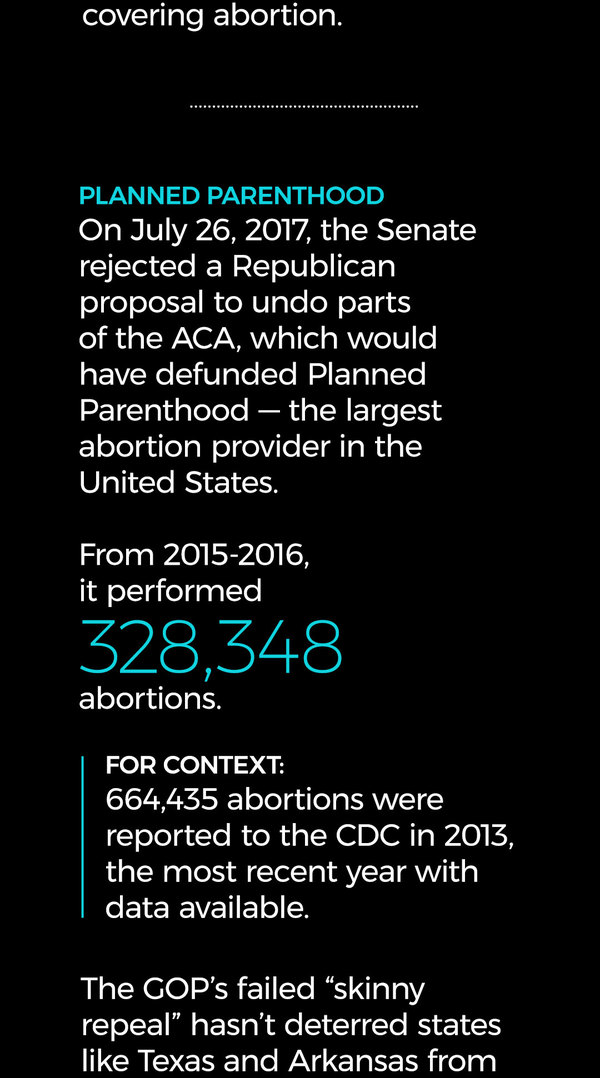
Planned Parenthood, the nation’s single largest abortion provider, has been at the center of flare-ups in Congress over abortion, health care, and federal funding since Republicans took control of the House of Representatives seven years ago.
Their work during the health care debate this year, said Robinson, reaffirmed the “grassroots-first” mentality set in November, but left the group seeking more long-term organizing.
“Now we’re ready to turn to a different phase,” she said.
The training work itself won’t exactly be a departure for Planned Parenthood. The group has trained thousands of “patient advocates” to deploy personal testimony in support of the Affordable Care Act and Planned Parenthood clinics, and hosted “Power of Pink” trainings for supporters. The “curriculum” they plan to use next month will be an updated version of one used they’ve used before, though never at a program of this scale.
“We’ve always had local organizers, activists, supporters, but not 1 million new supporters who are ready to come out and do the organizing work,” said Kersha Deibel, the group’s director of constituency organizing.
The 600 volunteer leaders, able to collaborate with local Planned Parenthood staff, will be autonomous, said Ganjaie, the Seattle-based field organizer, who has been helping plan the bootcamp trainings and identify top-tier volunteers to attend.
At each of the four gatherings, planned for Seattle, Phoenix, Charlotte, and Oklahoma City, around 250 hand-picked volunteers will undergo three days of trainings, covering digital programs, protests, congressional town halls, and the more basic work of building volunteer structures. Planned Parenthood will equip volunteers with online tools like phone banks and webinars, an official said, as well as “lots of pink materials, including shirts” — uniform of the “pink army” known to appear at rallies and protests.
As it stands, 600 of the 1,000 expected attendees will be chosen as volunteer leaders.
“We’re looking to pick out volunteer leaders who have naturally demonstrated leadership, folks who are already organizing on their own time,” said Ganjaie.
And after that, she said, they go home and “continue organizing.”
It’s more high-tech than holding signs and yelling. Opponents disrupt phone service, install wi-fi networks designed to confuse patients, and offer ultrasounds in RVs outside at least one clinic.
Throngs of anti-abortion protesters crowd the street in front of A Preferred Women’s Health clinic in Charlotte, North Carolina. The clinic, one of two abortion providers in the city, is regularly swamped by opponents who try to divert patients.
Pro Choice Charlotte
Religious imposition laws are designed to shield private individuals and businesses from complying with nondiscrimination laws based on a religious objection to that service.
Charlotte, North Carolina’s largest city, is at the center of a vicious battle between reproductive rights advocates and incredibly organized anti-abortion groups that launch regular massive clinic protests.
Such protests are far from new. Common tactics include standing outside (and often yelling at) clinics to threatening and sometimes attacking abortion providers.
But protesters at Charlotte’s clinics have begun adopting unorthodox tactics that includes the use of deafeningly loud sound and manipulation of online resources and search engine results.
Calla Hales, the administrator and co-owner of A Preferred Women’s Health Center (APWHC), which is the epicenter of the city’s current anti-abortion protest crisis, estimates that clinic staff began seeing an increase in protesters and a diversity of tactics in June 2016; that surge reflects 2016 National Abortion Federation statistics that reported more than 61,000 instances of picketing nationwide, the highest tally since the group began tracking anti-abortion violence and disruptions in 1977. Since last summer, the clinic has been a target for the ire of hundreds and at times thousands of protesters who block not only patients’ access, but also the neighboring health-care facilities in the business park where the clinic is located.
“There’s always been a protester presence here since this clinic opened in 2000, but it’s never been this hostile,” Hales said. “They’re in the street, they’re stopping cars, they’re saying hostile and inappropriate things on the loudspeakers.” It’s not clear why clinic protests ramped up, but the virulently anti-abortion group Operation Save America, which recently staged massive protests at Kentucky’s sole remaining abortion clinic, is headquartered in the Charlotte suburb of Concord. As a “descendant” of the radical anti-choice group Operation Rescue, the group has a decades-long history of anti-abortion mobilization, particularly blocking clinics.
The car-stopping and road-blocking constitutes a major facet of the issues at A Preferred Women’s Health Center, but it’s not the only one.
The protesters bring with them large RVs advertising ultrasounds (which are required for abortions in North Carolina, but are done within the clinic prior to the procedure) and noise amplifiers like that allow them to preach to clinic staff, patients, and clinic escorts and defenders.
What’s more, Hales says that officers with the Charlotte-Mecklenburg Police Department have been slow to respond to protester noise that exceeds acceptable levels stipulated by local ordinances. In the past year, she and her staff filed for thousands of sound permits to block protesters from utilizing speakers that would blare their anti-abortion messages. But the clinic has only been granted permits on less than ten occasions; clinic protesters received them the overwhelming majority of the time. The Charlotte-Mecklenburg Police Department could not be reached for comment about its handling of noise complaints. But the city recently changed the application process for sound permits, which could make the outcome more equitable.
Beyond concerns related to sound and the police, there are also issues with a wi-fi node for an open network named “Abortion Info.” Hales believes that one of the large RVs often parked outside the clinic is the home to the network.
Patients seeking internet access inside the clinic will often click the unsecured network, thinking it belongs to the clinic (which doesn’t have an open network due to security concerns). They are instead greeted by a log-in page whose design and logo resembles those of APWHC. To access the internet, people must watch a series of anti-abortion propaganda videos, and some who have logged onto the network reported to clinic staff that they later received calls, emails, and social media messages from people asking them if they need “guidance for abortion care.”
The cybersecurity concerns don’t end there. In March, the clinic’s network firewalls fell to “delay-of-service” attacks, where communications are slowed, often by flooding a system with thousands of false requests. These attacks increasingly target health-care facilities.
The delay-of-service attacks crashed APWHC’s phone and internet service and cost thousands of dollars in repairs. In an interview with the Charlotte Observer, the leader of Cities4Life, one of the main groups targeting the clinic, said that his group had nothing to do with the attacks and insinuated that Hales and clinic staff may have faked the attack for publicity. Since the March hack, Hales reported ten unsuccessful hacking attempts detected by their updated firewall.
Unfortunately, APWHC is not the only Charlotte abortion clinic that has fallen victim to cyberattacks from unidentified sources. According to clinic manager and counselor Sarah Shanks of Family Reproductive Health (FRH), someone not affiliated with the clinicchanged its Google business page earlier this year. The attacker changed the listing’s phone number to the clinic’s fax number and changed the login information, so for nearly three weeks, the clinic says it could not reach or be reached by patients calling its regular phone number.
“It was devastating to just hear the fax number ring all day, knowing it was maybe our patients or other people trying to reach us,” FRH’s Shanks said in the hallway of the quiet clinic.
Like APWHC, FRH also experiences some sound-related disruptions. There are fewer protesters at FRH due to location; APWHC is in a high-traffic, accessible business park, and FRH is tucked away in a more industrial neighborhood behind a large wooden fence and a barbed-wire one around the staff parking lot. That solid 6-foot-tall fence, however, doesn’t stop protesters from standing over it with an even taller ladder and a loudspeaker.
Beyond the physical presence and noise the protesters bring, there are also other, more sinister concerns at play. In an incident last fall, an anti-abortion protester made sure APWHC clinic escorts saw he carried a holstered gun though he did not pull it out; North Carolina allows licensed people to carry concealed weapons, but not the brandishing of those weapons. He fled from clinic security when confronted, only to circle the block slowly in his vehicle and park across the street. When the clinic called the police, Hales said a police officer dropped by but did not stop to speak with the man still parked across the street. Nothing more came of the altercation. Though the clinic called 911, Hales said there was no official report filed because no officers came to speak following the incident.
At both clinics, the anti-abortion protester presence has forced clinic staff and volunteers to the defensive—a move they say isn’t always conducive to caring for their patients. At APWHC, it forces them to do more work to counter their opponents’ moves, and sometimes that means resorting to more old-fashioned tactics.
Volunteer Diana Travis’ work with clinic defense includes building baffles around anti-abortion protesters’ sound amplifiers and constructing a 100-foot privacy wall out of black tarp and reinforced PVC pipes every Saturday. She expressed optimism that with sustained pressure from advocates, they can effectively counter protesters.
“I am hopeful things will change, but it’s going to be a long haul and will need constant monitoring,” Travis said.
After tortuous passage through congress, Michelle Bachelet’s bill legalising abortion in some circumstances will go before constitutional tribunal
A woman wearing a handkerchief embroidered with a uterus and the Spanish word for “free” participates in a pro-abortion march in Santiago, Chile. Photograph: Esteban Felix/AP
Chile is on the cusp of finalising a landmark ruling to legalise abortion under certain circumstances in a move that would signal a major victory for President Michelle Bachelet.
After two years of fractious debate, a bill that would permit termination of a pregnancy when a woman’s life is in danger, when a foetus is not viable or in cases of rape, could be passed this week.
Under existing law, women who have abortions and those who assist them face up to five years in jail, with hospitals obliged to report any suspicious cases to the police.
However, the bill faces a final hurdle after fierce opposition from the conservative right forced it to be referred to Chile’s constitutional tribunal.
Over the next three days, lawmakers and members of civil society will deliberate before a panel of eight male and two female judges. If endorsed, it will end Chile’s status as the last South American nation with an outright ban on abortion.
The deliberations coincide with the visit of Mike Pence, the US vice-president, who is visiting Chile as part of his South American tour. Pence is fiercely anti-choice, and is seen as highly influential in Donald Trump’s decision to reinstate an expanded, harsher version of the Mexico City policy.
Chile’s long-awaited reform would secure a key legacy for Bachelet, whose current term ends in March. The former head of UN women, who promised to push through the change when she took office for the second time in 2014, has faced a heavy backlash from the conservative right and the Catholic church. Some senators argue the measure violates the constitution, which protects the life of the unborn.
Demonstrations have been held across Chile this week in support of the bill.
Lilian Sepúlveda, a human rights lawyer and vice-president of the global legal programme at the Center for Reproductive Rights, said: “We are at the last significant step of what has been a two-and-a-half year process of advancing this progressive bill. At the end of the day you don’t know how a tribunal is going to rule but we are talking about very strong constitutional arguments in line with human rights.
“This bill is really testament to the response and hard work of women’s rights movements.”
Sepúlveda said she hoped the bill would pave the way for reproductive rights to be legalised on a wider scale.
“It’s a very important step in the right direction, but what we have to remember is the law covers three exceptions. In the longer run we still have a way to go for other women who may have social or economic grounds or other reasons for terminating a pregnancy.”
Chile legalised abortion for medical reasons in 1931, but the procedure was then banned without exception in 1989 as a parting shot from dictator Augusto Pinochet.
José Miguel Vivanco, from Human Rights Watch, will argue at the tribunal that the law is consistent with international human rights.
“Chile’s elite has fully embraced globalisation and a free market economy,” said Vivanco. “But the same elite that travels across the world engaging aggressively in business is, locally, extremely parochial, and will passionately defend views that are frozen in 19th-century rural society and universally challenged in the modern world.
“The law, unfortunately, is not going to allow abortion to protect the health of the mother. Only if her life is in danger will the law allow abortion, and then it will require the opinion of two doctors.
“There are very narrow constraints, and that is the result of very aggressive opposition from the right. It is extremely difficult to predict how the court will react.”
Michelle Bachelet delivers a speech at last year’s Ibero-American gender summit in Santiago. Photograph: Sebastian Silva/EPA
Pushing for change in the face of deep-rooted conservatism, Bachelet has faced a rift inside her ruling coalition and objections that the proposed legislation would lead to false rape claims.
However, after congress passed the law Bachelet wrote on Twitter: “Today, women reclaimed a basic right that we should never have lost: being able to choose when we’re living through painful moments.”
The bill is continuous with a wider regional shift to improve the reproductive rights of women. Colombia lifted an outright ban in 2006, while Uruguay – where the termination of pregnancies up to 12 weeks (14 weeks in cases of rape) was approved in 2012 – has led the way on decriminalising abortion.
But El Salvador is among South American countries where punitive ban remains, with women imprisoned even when they have experienced complications or miscarriages.
If legislation is relaxed in Chile, only a handful of countries worldwide, including Nicaragua and Malta, will still have an outright ban – or, as in Northern Ireland, rules so restrictive that they amount to de facto bans.
Last month, an opinion poll by the research firm Cadem found that roughly 70% of Chileans supported legalising abortion under the bill’s criteria.
Rights groups say 60,000 to 70,000 illegal abortions are performed each year in Chile. Between 2010 and 2014, nearly 500 people in Chile faced criminal charges in connection with abortions, according to the reproductive rights group, Miles.
The tribunal must make a final ruling before 28 August.
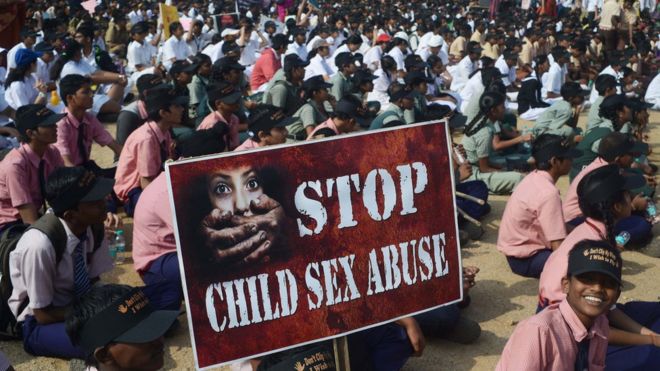
Image copyrightAFPImage captionIndia has a grim record of sexual assaults on children, with more than 10,000 raped in 2015
A 10-year-old rape victim who was denied permission for an abortion by the Indian Supreme Court last month has given birth to a baby girl.
The girl is not aware that she has given birth. During her pregnancy she was told her bulge was because she had a big stone in her stomach.
The baby weighing 2.2kg (4.8lb) was delivered by Caesarean section in Chandigarh at 09:22 (03:52 GMT).
Both the mother and the newborn are doing fine, an official told the BBC.
The girl alleges she was raped several times in the past seven months by her uncle, who has been arrested.
Her pregnancy was discovered in mid-July when she complained of stomach ache and her parents took her to hospital.
A local court in Chandigarh turned down the abortion plea on the grounds that she was too far into her pregnancy after a doctors’ panel said that termination of the pregnancy would be “too risky”. Later, the Supreme Court also refused to allow an abortion for her on similar grounds.
Baby ‘to be put up for adoption’
As the baby was born prematurely at 35 weeks, she has been placed in the neo-natal intensive care unit of the hospital where she will remain for the next few days, the BBC’s Geeta Pandey reports from Delhi.
The parents of the 10-year-old girl, who said from the beginning that they did not want to have anything to do with the baby, did not even look at the newborn, our correspondent adds.
The infant will be looked after by the child welfare committee until she is put up for adoption, an official said.
The girl who gave birth is expected to remain in hospital for up to 10 days.
Her case has dominated headlines in India for the past several weeks, with officials saying it is the first-ever case of a child so young giving birth.
Indian law does not allow terminations after 20 weeks unless doctors certify that the mother’s life is in danger.
But in recent years, the courts have received several petitions, many from child rape survivors, seeking to terminate pregnancies after 20 weeks. In most cases, these pregnancies are discovered late because the children themselves are not aware of their condition.
Child welfare activists who interact with the 10-year-old on a regular basis say that is precisely what happened with her – the girl is very innocent and had no idea what had happened to her.
Her parents also missed the telltale signs of her pregnancy perhaps because she’s “a healthy, chubby child”. Besides, they couldn’t imagine that their daughter could be pregnant at 10.
Image copyrightAFP
The scale of abuse in India
A child under 16 is raped every 155 minutes, a child under 10 every 13 hours
More than 10,000 children were raped in 2015
240 million women living in India were married before they turned 18
53.22% of children who participated in a government study reported some form of sexual abuse
50% of abusers are known to the child or are “persons in trust and care-givers”
WASHINGTON—The Trump administration is poised to issue a rule unwinding an Obama -era requirement that employee health benefits include contraception, which will spark a fresh round of litigation over an issue that has been before courts for six years.
Federal health officials are expected to finalize a regulation that would allow employers with religious or moral objections to birth control to omit coverage for contraception from their workers’ plans, according to two people familiar with its contents. The regulation closely mirrors an earlier, leaked draft, they said.
The Trump administration rule would allow a much broader set of employers to opt out of offering coverage for birth control, making moot a “workaround’’ designed by the Obama administration that allowed women in some cases to obtain coverage even if their employers had declined to offer it directly.
Based on early indications, the expected rule “would go a very long way to restoring religious freedom and conscience rights,” said Hillary Byrnes, assistant general counsel at the U.S. Conference of Catholic Bishops.
She said the rule couldn’t come soon enough. “We’ve been dealing with this mandate for over six years now,” she said. “A lot of people thought the administration would do something pretty quickly, yet here we are in August.”
Reproductive-rights activists say they will sue the Trump administration if it moves ahead with the rule, arguing that the change would unfairly impose employers’ beliefs on their workers and that the administration has cut regulatory corners in writing the policy.
“We are preparing various different legal theories to fight the rule very quickly,” said Mara Gandal-Powers, senior counsel at the National Women’s Law Center, an advocacy group. “We think we have a really strong claim.”
A spokeswoman for the Department of Health and Human Services declined to comment.
As a presidential candidate, Mr. Trump pledged support for Catholics and evangelical Christians who sued President Barack Obama and his top officials over the contraception requirement, contending that it forced them to violate their religious beliefs.
They also opposed a process, which the Obama administration dubbed an accommodation, in which an employer notifies the government of its unwillingness to cover contraceptives. That prompts the insurer administering the employer’s health benefits to assume the cost and administration of providing contraceptives, effectively cutting out the employer.
Religious employers challenged the policy in court, saying it made them complicit in a sin. The Supreme Court last year sent the case back to lower courts.
The Trump administration plans to offer the plaintiffs precisely what they sought: an exemption from the contraception requirement for all employers who want one, according to people familiar with the plan, ending the need for litigation.
Others regard the expected rule as a step back in a decadeslong fight to secure women’s access to contraceptive care.
Lawyers preparing potential legal cases for opponents of the change say that if the rule resembles the leaked draft, the policy could qualify as sex discrimination, since it would disproportionately affect women’s health care. They also plan to argue that leaving a decision on contraceptive coverage to employers could amount to religious discrimination by subjecting workers to the beliefs of their employers.
“If the rule says any employer can withhold this benefit from employees, then you have a whole set of questions about whether the government is enabling employers to impose their beliefs on others,” said Louise Melling, deputy legal director at the American Civil Liberties Union.
People familiar with the proposed rule say the Trump administration plans for it to take effect as it is published. Nicholas Bagley, a University of Michigan law professor who has analyzed much of the health-law litigation of the last six years, has said that could open the administration to lawsuits for implementing the rule without time for public comment and consideration.
“The argument they make is, ‘We’ve thoroughly vetted this issue, and we’re only making a minor change,’” he said. “If that was true, that argument would hold water. But that’s not true in this case.”
















































Northern Ireland’s Department of Health has declined to issue new guidance on abortion to doctors and other health professionals because “there has been no change to the law on abortion”. This is despite the fact that the situation clearly has changed since women from the region can now access free, NHS abortions in England.
This stubborn refusal to recognise the reality of women’s reproductive healthcare needs is concerning because it ignores the fact that, at present, GPs in Northern Ireland are not permitted to purchase procedures outside Northern Ireland “that would be illegal in Northern Ireland”. This prohibition clearly needs to be updated to take account of the new situation.
Since the end of June, women from Northern Ireland can receive free NHS abortions through self-referral to the British Pregnancy Advisory Service or Marie Stopes; these agencies will then recoup the costs from the Equalities Office. Leaving aside the cost, financial and emotional, of having to travel for healthcare, this should work well for women who need an abortion mainly because they do not want to be pregnant.
But a small minority of women need, for medical reasons, to have their terminations in a hospital setting. With only 16 abortions carried out in Northern Ireland by health professionals in 2014-15 and again in 2015-16, clearly women with a range of health issues are not able to access legal abortions in Northern Ireland. Until now, they have had to take their chances in organising their own terminations at clinics that are not equipped to deal with serious medical conditions.
If nothing else, GPs need to be informed of care pathways through which these women can end their pregnancies in hospitals where all their medical needs can be met. It was to help such women that the idea of NHS-funded abortions for women from Northern Ireland first arose.
After the 1997 general election, hopes were high that the 1967 Abortion Act would be extended to Northern Ireland, particularly since both Tony Blair and Mo Mowlam, then secretary of state for Northern Ireland, had voted while in opposition for the extension of the act. However, it soon became clear that women’s rights were to be sacrificed to the “peace process”. Mowlam later admitted she “would have liked to have done something” for women in Northern Ireland but could not – for fear of “stirring up the tribal elders”.
Together with Voice for Choice, campaigners in Northern Ireland began to look at free NHS abortions as a stopgap measure that would reduce the inequality of access a little.
In February 1999, Maria Fyfe, then Labour MP for Glasgow Maryhill, wrote to Mowlam about abortion law in Northern Ireland. Adam Ingram, then a minister of state in the Northern Ireland Office, replied on Mowlam’s behalf on 10 March 1999. He wrote: “You raised the possibility of arrangements being introduced to enable GP fundholders and their purchasing authorities in Northern Ireland to fund terminations of pregnancy carried out elsewhere in the United Kingdom. I understand that such arrangements would not be possible in the case of fundholders who … are specifically prohibited from purchasing treatment for their patients outside Northern Ireland which would be illegal in Northern Ireland, such as termination of pregnancy.” (Of course, termination of pregnancy is the only treatment available in the NHS which would be illegal in Northern Ireland.)
The Northern Ireland assembly has shown itself incapable of dealing with the reality of abortion in the region. Debates have tended to be high on anti-abortion rhetoric and low on practical approaches to the reality of women’s lives in the 21st century. For almost 20 years now, Westminster has looked the other way. Indeed, a letter sent at the end of June from Justine Greening, the minister for women and equalities, to MPs – setting out the government’s proposal to provide NHS abortions to women from Northern Ireland – ended with an assurance that “none of this changes the fundamental position that this is a devolved issue in Northern Ireland … This announcement does not change that position”.
Women in Northern Ireland continue to be discriminated against. Westminster cannot devolve human rights; it remains the guarantor of such rights despite devolution. The (non-)response of the Northern Ireland Department of Health to the changed situation reinforces the view that Stormont is incapable of bringing women’s rights into the modern era and ensuring full reproductive healthcare in local hospitals.
The move to give everyone access to NHS abortions in Britain is a step in the right direction, but it is only the first step. Now Westminster needs to act to end half a century of inequality for women in Northern Ireland.
https://www.theguardian.com/commentisfree/2017/aug/22/women-northern-ireland-abortion-reproductive-rights-westminster-change-law?utm_content=buffer06596&utm_medium=social&utm_source=facebook.com&utm_campaign=buffer