Republican members of Congress continue to push the false narrative that medication abortion—especially through telemedicine methods—is unsafe and poorly regulated.

A 2018 report from the National Academies of Sciences, Engineering, and Medicine found that serious complications from medication abortion are rare.
Shutterstock
U.S. Rep. Ron Wright (R-TX) introduced a bill last month that would impede access to medication abortion through telemedicine and punish health-care providers with heavy fines and possible prison time. It comes weeks after another conservative member of Congress introduced a bill focused on medication abortion.
The Teleabortion Prevention Act of 2019 (HR 4935) was introduced on October 30. It would make it a federal offense for a health-care provider who provides medication abortion to do so without a physical examination of the patient, “without being physically present at the location of the chemical abortion,” and without scheduling a follow-up visit that happens 14 days after the administration of the medication abortion. The health-care provider could be fined up to $1,000 or imprisoned for up to two years, or both, under this legislation.
The bill repeatedly refers to medication abortion as “chemical abortion,” a term used by anti-choice organizations such as March for Life, National Right to Life Committee, and the Susan B. Anthony List. The latter two groups endorsed the legislation. “The use of the term ‘chemical’ as opposed to ‘medication’ is meant to spread the lie that medication abortion procedures are not medical in nature,” said Nimra Chowdhry, state legislative counsel at the Center for Reproductive Rights.
The bill appears to be part of a broader, sustained strategy from anti-choice lawmakers and organizations across the country to portray medication abortion as unsafe through misinformation and overregulation of medication that has a 19-year safety record.
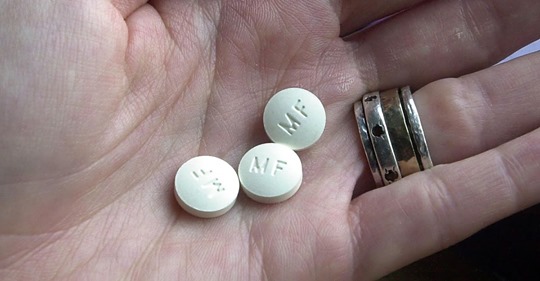
Medication abortion requires that a patient take two pills, mifepristone and misoprostol. It is commonly used for abortion at or under ten weeks after the first day of a patient’s last period. A 2018 report from the National Academies of Sciences, Engineering, and Medicine found that serious complications from medication abortion are rare. The report found “no evidence” to suggest state regulations of medication abortion “improve safety or quality of care,” according to the National Academies.
Many patients in rural areas of the country where clinicians may be inaccessible require the use of telemedicine methods for medication abortion. This involves clinicians speaking with patients through a video conference, considering patient health records, and authorizing the medication remotely. According to a 2017 report from the American Congress of Obstetricians and Gynecologists, around half of U.S. counties didn’t have an obstetrician-gynecologist in 2010.
But Republican members of Congress continue to push the false narrative that medication abortion—especially through telemedicine methods—is unsafe and poorly regulated.
“Although we currently have protections in place, pro-abortion groups are looking to get around the law. There is evidence that teleabortion participants are not getting appropriate medical advice or assistance, and ending up severely injured,” Rep. Wright said in a statement on the bill that did not offer evidence to back up his claim.
Wright’s bill follows the introduction of Rep. Robert Latta’s (R-OH) HR 4399, the Support and Value Expectant Moms Act of 2019 in mid-September. This bill would prevent the dispensation of medication abortion pills by telemedicine or mail. Under the legislation, the U.S. Food and Drug Administration (FDA) would also be prevented from approving new medication abortion drugs and making labeling changes for already approved drugs. Latta in a statement on the bill made a similar false claim to Wright that medication was “dangerous,” and that there wasn’t “proper medical oversight” of medication abortion.
Chowdhry said the introduction of the bills should come as no surprise. By attacking medication abortion access, anti-abortion groups and lawmakers can place barriers to abortion on all sides.
“Taken together, these bills attack how patients access abortion care while overregulating the medication itself,” she said. “This comes at a time when states are rapidly restricting access to abortion care, and telemedicine is improving access—so we are not surprised that this type of policy has become a new focus for federal lawmakers.”
Chowdhry added that the strategy of these bills appears to be a “calculated push” by federal lawmakers, anti-choice groups, and anti-choice state legislators to spread misinformation about medication abortion and make it more difficult to access the procedure.
This has already happened on the state level. Several states have enacted requirements mandating misinformation about medication abortion, forcing doctors to falsely tell patients that it’s possible to reverse a medication abortion as part of pre-abortion counseling. Kentucky, Nebraska, Oklahoma, and North Dakota legislatures enacted those requirements this year. (The latter two aren’t in effect after courts temporarily blocked them.) Arkansas passed such a requirement in 2015; it passed another law in March 2019 specifying that the “abortion reversal” notification must be in writing.
Bans on administering medication abortion through telemedicine are also widespread. According to the Guttmacher Institute, “34 states require clinicians who perform medication abortion procedures to be a physician” and “18 states require the clinician providing a medication abortion to be physically present during the procedure, thereby prohibiting the use of telemedicine to prescribe medication for abortion remotely.”
“The introduction of this type of legislation highlights how anti-abortion lawmakers want to spread lies both through legislation and regulation, even though medication abortion is routinely, and safely provided nationwide,” Chowdhry said.