A fund in Georgia is responding to restrictive legislation with a familial kind of care.

Oriaku and Dirichi Njoku, of the abortion fund arc-Southeast.Photograph by Andrew Lyman for The New Yorker
n June, 1994, at a pro-choice conference in Chicago, twelve black women gathered together to talk. One, Loretta Ross, was the executive director of the first rape crisis center in this country. Another, Toni Bond, was the executive director of the Chicago Abortion Fund. A third, Cynthia Newbille, was the leader of the National Black Women’s Health Project, which was among the first national organizations to be devoted to the wellness of black women and girls. After the first day of the event, which was hosted by the Illinois Pro-Choice Alliance and the Ms. Foundation, the group met in a hotel room. “We did what black women do when we’re in spaces where there are just a handful of us,” Bond, who is now a religious scholar, recalled. “We pulled the sistas together and talked about what was missing.”
Abortion had been decriminalized in 1973, with the Supreme Court’s Roe v. Wade decision, but, with the passage, in 1977, of the Hyde Amendment, which banned federal funding for almost all abortions, the procedure had become too expensive for many women. In 1993, Bill and Hillary Clinton had proposed an overhaul of the health-care system, but reproductive-health coverage was sacrificed to make the reforms more palatable to Republican lawmakers. To the women in the hotel room, the conversation at the conference about reproductive health focussed too narrowly on “choice.” There had been no discussion of the services that black women needed most, such as fibroid-tumor screenings, mammograms, and pre- and postnatal care. (Black women have a higher risk of fibroids than white women, higher percentages of late-detected breast cancer, and a maternal-mortality rate that is more than three times higher.) Nor was there an acknowledgment that the reproductive and parenting decisions of black women were limited by poverty, unequal pay, lack of access to adequate housing and schools, and the abuses of the policing and criminal-justice systems.“No one was talking about black women’s health as a whole,” Ross told me, not long ago. “Too many people were examining policies through the lens of white supremacy.”
The women created the term “reproductive justice” to describe the scope of their activism. They were inspired by the work of the black legal scholar Dorothy Roberts, whose research traced the history of efforts in this country to control black women’s reproductive freedom, beginning with the forced procreation of enslaved women. Abuses had continued into the nineteen-seventies, when thousands of women—including some who were receiving public assistance in North Carolina and others who were incarcerated in California—were involuntarily sterilized. In Arizona, South Carolina, Tennessee, and Washington, state-court judges often offered black female defendants reduced prison sentences if they agreed to get birth-control shots or implants. (This practice was happening as recently as two years ago.) As Roberts observed, black people had turned to their families, friends, and neighbors for the family-planning services and child care that the government had denied them. Bond said, “Reproductive justice offers us an opportunity to talk about the ways in which black women have exercised agency and been resilient even in the midst of reproductive and sexual oppression.”
The twelve women called themselves Women of African Descent for Reproductive Justice. After the meeting in the hotel room, they bought full-page ads in the Washington Post and Roll Call, publishing a letter to Congress that argued for “unimpeded access to abortion as part of the full range of reproductive health services offered under health care reform,” which should be available “regardless of ability to pay, with no interference from the government.” The letter stressed that reform should be comprehensive, and “must include strong anti-discriminatory provisions.”
During the following months, Ross and some of the other women led a reproductive-justice discussion in Cairo, Egypt, and wrote a public letter in support of Joycelyn Elders, the former Surgeon General, whom Bill Clinton had asked to resign after she said that she approved of educating children about masturbation to avoid the spread of aids. In 1997, with funding from the Ford Foundation, sixteen groups representing African-American, Asian-American, Pacific Islander, Latina, and indigenous women came together to form SisterSong, a national collective advocating for the reproductive and sexual health of women of color. SisterSong was based in Atlanta, the birthplace of the civil-rights student protests and the home of several historically black colleges; the city also had the largest black gay population in the South. Activists there had already created a parallel system of care, encompassing the Feminist Women’s Health Center, an abortion and gynecological clinic in the North Druid Hills, which grew out of a women’s self-help health group, in 1976; the National Black Women’s Health Project (now the Black Women’s Health Imperative); and SisterLove, founded, in 1989, to tackle H.I.V./aids.
In the next few years, the leaders of SisterSong and of newer reproductive-justice organizations—such as Spark Reproductive Justice Now, founded, in 2007, to include queer perspectives in the movement—held round-table discussions and met up for dinners and happy hours, as well as get-togethers at Charis Books, a feminist bookstore downtown. In 2004, after the passage of the Partial-Birth Abortion Ban Act, SisterSong, Planned Parenthood, and the National Organization for Women, among other groups, put together the March for Women’s Lives on the National Mall in Washington, D.C. In 2010, after the passage of the Affordable Care Act, several Atlanta-based reproductive-justice groups sent their members to D.C., to protest the Stupak-Pitts Amendment, which aimed to prevent federal funds from being used to pay for insurance plans that covered abortions. The current Democratic Presidential candidate Julián Castro, one of several politicians who have recently spoken about the importance of reproductive justice, told me that he was thankful to the Atlanta community who had launched the movement. “Their voices are crucial, especially now, to get us out of our comfort zone,” he said.
Oriaku Njoku was twenty-five when she visited Atlanta, in October, 2010, to attend the Atlanta Pride Festival. The daughter of middle-class Nigerian immigrants, Njoku had grown up in a mostly white neighborhood in Bowling Green, Kentucky. While attending the University of Kentucky, she came out to her siblings, then to her parents, and participated in L.G.B.T.Q. activism. After graduating, she worked in retail in Kentucky and Indiana. At the Pride celebrations, she was drawn to Atlanta, with its ambitious black residents and its queer scene, and moved there a few months later. In January, 2013, she attended an event held by Spark that was an introduction to reproductive-justice organizing, and later volunteered on a Spark initiative to stop the practice in Georgia prisons of shackling pregnant women during childbirth. “Doing reproductive-justice work has been the one place where I feel like I can bring my full self to the table,” she told me recently. “Being a first-generation queer black Southern fat femme, I can bring all those identities to work and do it unapologetically.” Njoku, who is now thirty-four, calls herself “a giver.” She has the Southern female tendency to go out of her way to put others at ease, filling in an awkward silence with a caring question, a compliment, or a wavering “um.” When she is frustrated, she is just as accommodating, but her voice takes on a slight edge. She likes to wear Igbo dresses and head wraps in vivid colors, and has a sprawling tattoo on her forearm that reads “Love is lifeforce”—a quote from the queer Jamaican-American poet and activist June Jordan.
After the 2013 Spark event, Njoku started travelling to other reproductive-justice gatherings, including the annual summit held by the National Network of Abortion Funds, where people talked about intersectionality and abortion access. She briefly dated a trans man, a human-rights defender from Uganda, who was seeking asylum and trying to bring his children to the United States; she realized that trans men also had trouble exercising their reproductive rights. She began to ask people for their gender pronouns.
In February, 2014, Njoku got a job taking patients’ information and making appointments at the Atlanta Women’s Center, an abortion clinic near the wealthy enclave of North Buckhead. As of that year, legislatures in Georgia and twenty-five other states had enacted laws restricting the coverage of abortion in the Affordable Care Act health-insurance marketplaces. Women who contacted the clinic were often struggling to come up with the money for their abortions, which became more expensive as their pregnancies progressed.
Njoku regularly directed such women to call the National Abortion Federation, which, in 2014, donated to more than a hundred thousand women based on their needs, with the expectation that the women would raise as much as they could themselves. Its hotline was often busy for hours on end. When Njoku looked for regional sources of assistance, she discovered only one in Georgia: the Magnolia Fund, which helped women pay for abortions performed at the Feminist Women’s Health Center. (Magnolia closed last year.)
In May, 2014, Njoku and two colleagues decided to set up their own abortion fund to help women in Georgia, Alabama, Florida, Mississippi, South Carolina, and Tennessee. “I was, like, We gotta do right by our people,” she recalled. “There’s no reason that our folks should be calling multiple numbers and waiting on hold forever to try and get in touch with someone for basic health care.” Kwajelyn Jackson, of the Feminist Women’s Health Center, called abortion funds “the conduit through which people are going to be able to get connected with care in the long run.” That November, Njoku took a job at Summit Medical Associates, assisting in the operating room and caring for women in post-abortion recovery. Meanwhile, she approached the National Network of Abortion Funds for advice. Njoku and her colleagues worked from coffee shops and buffet restaurants, applying for grants and organizing fund-raisers, including a fish fry. Their fund, Access Reproductive Care-Southeast, began operating in May, 2015. Its first grant paid for a headquarters, in an airy arts center in downtown Atlanta. By January, 2016, Njoku was working there full time.
The following spring, Njoku went on a tour of the Deep South, hoping to form relationships with employees at independent clinics, which, in that part of the country, are more numerous than Planned Parenthood centers. At each one, she made note of the affordable hotels nearby, the schedules for intakes and procedures, waiting lists and patient backlogs, and whether there were translators on hand. The fund set up a hotline in July, 2016. As it received more calls, she needed more volunteers to take women to and from appointments. (Clinics require that women receiving sedation have someone with them to take them home.)
That year, arc-Southeast gave funding and assistance to about fifty women each month; it now serves more than three hundred a month. The average cost of an abortion is around five hundred dollars, with later-term abortions sometimes in the thousands of dollars. arc-Southeast gives most women between seventy-five and a hundred dollars. The fund now employs a staff of seven, who are mostly black and queer, and has more than a hundred volunteers. They provide a kind of care that might be considered familial, booking travel and hotel rooms, taking women out for meals, and even putting them up for a night or two in their own homes. “We try to lead with love,” Njoku said. In 2017, Njoku’s sister Dirichi, who goes by Chi Chi, joined the organization to run the hotline. A former nurse, Chi Chi had little knowledge of reproductive justice, but she felt a connection to the fund’s mission. When she was nineteen, she got pregnant after being raped by a friend and had an abortion, an experience she often shares with callers.
arc-Southeast has found rooms for homeless women who would otherwise have spent the night outside the clinic, and counselled mothers and daughters who needed abortions at the same time. Not long ago, the fund referred an undocumented Honduran woman living in Atlanta with her two children, whose husband had been detained by Immigration and Customs Enforcement, to the National Abortion Federation, which agreed to pay for her procedure. The woman was twenty-six weeks pregnant, six weeks past the limit for abortions in Georgia. She could have taken a bus to a state where the gestational limit was higher, but she’d heard that immigration raids on buses were common. Njoku decided that the fund’s hotline operator, Crystal Zaragoza, who had previously run a clinic for queer migrants in Phoenix, should drive the woman in a rental car to a clinic in Bethesda, Maryland. Zaragoza and the woman stayed in an Airbnb for four days. The fund paid more than a thousand dollars for the car, the accommodation, the woman’s medication, and care for her children while she was away.
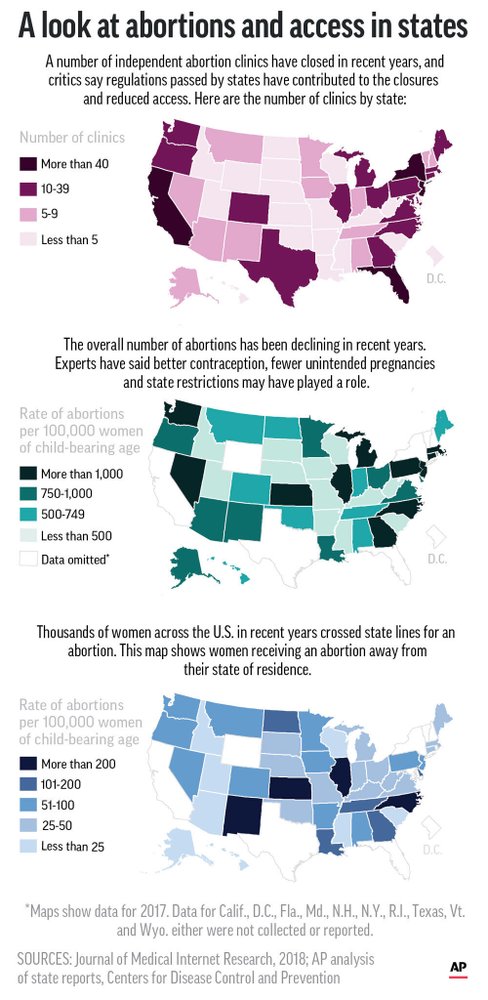
Abortion in Georgia is legal up to the twentieth week of pregnancy, and fourteen of the state’s seventeen clinics are in the Atlanta area. Calls come in to the fund from all over the Deep South; for some women, the clinics near them have closed, or offer only limited services. In South Carolina, there are just three abortion clinics. In 1995, the state put into place regulations requiring that all clinics terminating second-trimester pregnancies meet the same design and construction standards as “ambulatory surgical facilities.” Ostensibly meant to insure women’s safety, the regulations dictated, in overwhelming detail, specifications including the width of the corridors, the number and size of procedure rooms, and the size of the janitor’s closet. Pro-choice organizations and physicians agreed that the regulations were politically motivated; the necessary changes would be too costly for most clinics to make, and, ultimately, they would do little to improve patients’ care. More than half of the South Carolina women who had abortions in 2017 travelled outside the state for their procedures.
Spring is the fund’s busiest season. (As Chi Chi put it, “People get it on in the winter.”) In April, 2018, arc-Southeast assisted a hundred and eighty-two women. This past April, it helped three hundred and ninety-seven callers, and Njoku spent much of her time in her car. One morning, she woke up early to pick up a woman from her home in south Atlanta and took her to the Atlanta Women’s Center, in the northeast of the city. There, she met up with another woman, who was accompanied by her partner and their child, and gave her cash for food and a hotel. Then she took the first woman home and headed back to the office. In the parking lot, she received a call from Chi Chi about Naomi (a pseudonym), a woman who was waiting at Summit Medical Associates, four miles away, in need of an escort. Naomi had driven more than two hundred miles that morning, from Columbia, South Carolina, for her appointment. She believed that she was fourteen weeks pregnant. Twenty minutes after the call, Njoku arrived at the clinic and signed Naomi in. The process for second-trimester abortions, known as “dilation and evacuation,” usually takes place over two days. After the first appointment, Njoku gave Naomi a ride to her motel and learned that she and her partner were not speaking, that her best friend had wanted her to have the baby, and that she hadn’t told her parents she was pregnant, because she was too ashamed. Naomi knew that she needed an escort, but another friend, who had agreed to accompany her, had cancelled at the last minute. She had hoped to persuade the clinic to make an exception.
When I recently talked to Naomi, she still hadn’t told her family about her abortion, and she said she would take the secret of it to the grave with her. On her first night in Atlanta, she recalled, she had been in pain and lonely, and had slept badly. In the morning, when Njoku picked her up for her second appointment, Naomi was amused to see Njoku’s Pomeranian-Shiba Inu mix, Marley, in the passenger seat. She felt comforted by Njoku’s presence. “I didn’t have nobody there with me, and just in the moment of time being in that car with her—that really meant a lot,” Naomi said.
This past spring, after the confirmation of Brett Kavanaugh to the Supreme Court, in October, 2018, legislatures in Alabama, Arkansas, Georgia, Kentucky, Louisiana, Mississippi, Missouri, Ohio, and Utah all passed bills that placed restrictions on abortion, which were intended to undermine Roe v. Wade. In May, Alabama passed a bill that, if it goes into effect, would outlaw abortion, even when pregnancies are the result of rape or incest, except in cases where the mother’s life is at risk; doctors who performed the procedure could go to jail for up to ninety-nine years. The new law is being challenged in federal court by the American Civil Liberties Union and Planned Parenthood on behalf of Alabama abortion providers.
In Georgia, a “heartbeat bill” was passed, banning abortion after about six weeks—before most women know that they are pregnant. In June, the A.C.L.U., the A.C.L.U. of Georgia, the Center for Reproductive Rights, and Planned Parenthood filed a lawsuit, representing SisterSong, Georgia medical providers, and their patients, arguing that the law disproportionately affects people of color and rural and poor residents. Stacey Abrams, who ran for governor of Georgia on a platform that included a call for reproductive justice, described the law, on Twitter, as “a forced pregnancy bill.”
When I visited the arc-Southeast office this summer, Njoku and Chi Chi were worrying about the bill, too. “I’ve probably only had one or two callers who were under six weeks, and that scares me,” Chi Chi said. “Because, when this law happens, what’s going to happen with all these other women? How’s it going to be like next year when these women call me and I have to tell them that they can’t do this? Abortions aren’t going to stop, even if they make them illegal. And then I wonder, Well, what’s going to happen to me? Am I going to get in trouble because I’m helping these women? I told my sister, ‘I’ll go to jail. I want you to keep fighting for this.’ ”
In May, Njoku and her colleague Quita Tinsley made the same tour of clinics that Njoku had in 2016, anxious to see how abortion providers were faring in the aftermath of the legislation. At the West Alabama Women’s Center, in Tuscaloosa, the director, Gloria Gray, a gruff, kind woman in her sixties, wearing dark-blue scrubs, greeted Tinsley and Njoku in the reception area. She showed them into her office, which was decorated with pictures of her grandchildren and Alabama football mementos. Affixed to the back of her computer monitor was a bumper sticker that read, “If you still support Trump, stay 500 feet behind. I don’t trust your judgment.”
Gray and Njoku talked about the recently signed Alabama abortion law. Njoku explained that many callers to the fund assumed that it had already gone into effect. One woman living in Gulf Shores had called all the clinics in her area and discovered that they had closed. She had surmised that the ban was to blame. But the closures were more likely due to a range of licensing requirements known as the Targeted Regulation of Abortion Providers (trap) laws, which have been passed by the health departments of Republican-controlled state legislatures since the nineties. As in South Carolina, the stipulations in trap laws are cumbersome, usually having little to do with medical necessity, and, in recent years, they have become more onerous. In ten states, including Alabama, Florida, Texas, and Mississippi, doctors performing abortions are required to have admitting privileges or similar arrangements at a nearby hospital—privileges that some hospitals, for political or budgetary reasons, refuse to grant. As a result of various trap laws, the number of clinics in Alabama has declined from twenty in 1992 to just three. In 2016, the Supreme Court struck down Texas’s law requiring that any doctor performing an abortion have admitting privileges and that clinics be set up as ambulatory surgical centers; the decision, in Whole Woman’s Health v. Hellerstedt, deemed that the requirements placed an “undue burden” on people seeking access to abortions and were therefore unconstitutional. Last week, the Court said it would hear arguments in a case from Louisiana that is nearly identical, raising concerns that the 2016 decision will be overturned.
In 2015, Gray hired the renowned abortion doctor Willie Parker to replace the clinic’s former physician, who had retired. Parker—a well-known Christian reproductive-justice advocate, who has been honored by the United Nations Office of Human Rights and by Planned Parenthood for his work in Mississippi and Alabama—applied to the local hospital for admitting privileges, but was not granted them. The clinic had to shut down for eight months. It filed a lawsuit, and reached a settlement on the admitting-privileges requirement. But Gray said that she had sensed an unwelcoming atmosphere at the hospital ever since. The West Alabama Women’s Center was often surrounded by protesters; one of them, Gray noticed, was the wife of a doctor at the hospital. Abortion is a safe procedure, but, in the rare case that a woman experiences complications, she needs to go to the hospital. “I hate to send a patient out there and not know how she’s being treated,” Gray said. As a result, at the end of 2015, Gray decided that the center would stop providing abortions to women who were past the seventeenth week of pregnancy. A clinic in Huntsville, about a hundred and fifty miles away, was now the only one in the state that did late-term abortions.
Some obstacles had arisen from less expected places. In March, the Alabama reproductive-rights scene was shaken when Parker, who had also worked in the Huntsville clinic since 2016, was accused by the reproductive-rights activist Candice Russell of sexual assault. He denied any misconduct, but resigned his chairmanship of the board of Physicians for Reproductive Health. “We lost a very high-profile, vocal person who spoke out on women’s rights, because everybody is cancelling his speaking engagements now, and that’s unfortunate,” Gray said.
The day after the stop in Tuscaloosa, Njoku and Tinsley visited the Huntsville clinic, which was homey, with lilac walls. “It’s nice to finally meet,” the receptionist said. “Y’all send us funds—you got to know who you’re working with, honey.”
The clinic has a majority-black staff. The full-time physician, Yashica Robinson, who was polished even in scrubs, with dark, curled hair and elegant jewelry, greeted the women warmly. “Dr. Parker says this is Wakanda,” she said. She led Njoku and Tinsley into a tidy linoleum-floored break room, where she and Dalton Johnson, who started the clinic, in 2001, were having lunch. The Huntsville center was the last abortion clinic to have been certified in the state; trap laws had made opening new clinics prohibitively expensive and difficult.
“The main thing with us is the constant financial strain,” Johnson told Njoku. In March, a man had sued the clinic, claiming that when his girlfriend had had an abortion there, two years earlier, he had not given her permission to do so, and calling the termination a “wrongful death.” A county probate judge allowed the suit to proceed under the “personhood” amendment to Alabama’s constitution, which passed in November, 2018, with the intent of “declaring and affirming the public policy of the state to recognize and support the sanctity of unborn life and the rights of unborn children.” Johnson said that, in April, the clinic had paid its lawyers fifteen thousand dollars in retainers.
Robinson joined the clinic in 2005, and in 2013 she applied to Huntsville Hospital for admitting privileges. The hospital stalled for such a long time that she hired a lawyer to push her case. The privileges, when they were granted, meant that she had to be within a thirty-minute drive of the hospital at all times in order to keep them. This is standard for ob-gyn providers in the area, and other doctors had formed groups to cover one another’s shifts, so that they could travel, but they excluded Robinson. Some of them did not want “the lady who does abortions” to deliver their patients’ babies, Robinson said; others were afraid of attracting protesters to their offices. She was desperate to hire another doctor for the clinic. She laughed, darkly. “It’s going to take somebody with a strong backbone to come and join us, and to put up with all it takes to live and work in this community,” she said.
After the passage of the Alabama and Georgia restrictions, in May, Senators Bernie Sanders and Kirsten Gillibrand and the comedian Kumail Nanjiani encouraged their Twitter followers to donate to abortion funds, praising the work of arc-Southeast and Yellowhammer, a fund that a University of Alabama graduate, Amanda Reyes, had co-founded, in September, 2017. By mid-July, arc-Southeast received more than three hundred thousand dollars in donations. Yellowhammer, which funded three hundred and thirteen abortions in 2018 and is extremely active on social media, received more than two million dollars; it had not taken in as much in its entire existence before then. The singer Maggie Rogers pledged profits from her merchandise sales, and, in July, Pussy Riot played a sold-out concert in Birmingham benefitting the fund and Planned Parenthood.
While Njoku and Tinsley were in Tuscaloosa, they went to supper at a Tex-Mex restaurant with Reyes and some of her employees, including Candice Russell, the activist who had accused Parker of assault, who had recently joined the Yellowhammer staff. We all introduced ourselves, giving our preferred pronouns. The pro-choice movement, Russell said at one point, used the term “reproductive justice” too freely. Russell referred to Yellowhammer’s work with “underhoused” people, a near-synonym for “homeless” that Njoku and Tinsley later confessed they had never heard before. The dinner was surprisingly tense, with the Yellowhammer staff mostly ignoring their peers at arc-Southeast, and Reyes focussing her attention on me. Later, when I asked Njoku about the tension, she shrugged it off, saying that she still hoped the funds would continue to work together on the cases of people in Alabama.
In June, the local news outlet AL.com published a story in which the directors of Alabama’s three abortion clinics and a former Yellowhammer board member complained that Yellowhammer had used its donations for inflated salaries and unnecessary purchases. Reyes denied the claims, saying that the money was being spent appropriately. When I asked Reyes about the complaints, she said, “Things moved so fast, and the speed at which we went from a really small organization with an all-volunteer workforce to becoming an organization that was poised to be so much more . . . resulted in those misunderstandings.” Since then, she said, Yellowhammer had sought management advice and had hired a communications firm.
Njoku was glad that the abortion bans were inspiring people to donate and to volunteer. On social media, people were posting selfies of themselves wearing “Everyone Loves Someone Who Had an Abortion” T-shirts. Now everyone was an “intersectional feminist,” she said. But there was a danger, she thought, that people would forget the black women who had founded the movement to address ongoing injustices. “It’s not because it’s cute or because it’s sexy or because Stacey Abrams said ‘reproductive justice’ in the State of the Union response,” she said. “It’s because it’s real.”
One Monday morning in June, Njoku and Chi Chi were training a new intern, Imani, a sophomore at Clark Atlanta University, to answer the hotline. Slight and bespectacled, Imani grew up in the Bronx and attended an all-girls Catholic school, where talk of sex and abortion was “hush-hush.” She had become a convert to reproductive justice after attending a conference hosted by the advocacy group Civil Liberties and Public Policy.
Njoku pulled up on her computer screen the voice mails that had been left over the weekend. She and Chi Chi have a teasing rapport, and make videos of themselves as Nigerian aunties who critique rap lyrics, a pastime that often makes its way into the office. “Are you starting from the bottom, now we’re here?” Njoku asked Chi Chi, quoting a lyric from a song by Drake.
Chi Chi said that she was; Njoku would start from the messages at the top of the list. Imani scooted her chair over to Njoku’s screen. Njoku turned on one of the Samsung Galaxy phones they use for the hotline. “This is the trap phone,” she said, referring to the prepaid cell phones typically used by drug dealers. Imani laughed.
Part of the job, Njoku explained, was to help callers by brainstorming how to “hustle” for the money they needed. They encouraged women to ask their family and friends for help with their abortion fees just as they would if they had any other bill they couldn’t pay. “Just because there’s shame and stigma around it doesn’t mean we can’t still use that same energy to make sure you get what you need,” Njoku said. Chi Chi added, “It’s sort of like, ‘We’re your friend—we’re your friend who you never met who will steer you in the right direction.’ ” She and Chi Chi often call clinics on behalf of patients who are a hundred or so dollars short of the total fee and ask the staff to see them anyway. More often than not, the clinics agree.
Njoku returned the call of one woman whose parents were against the idea of abortion, and urged her to ask to borrow money from them anyway. “Folks don’t need to know all your business, you know?” she said. “It’s enough to be, like, ‘Hey, I’m needing some help right now. Y’all think that you can lend me a little bit?’ ”
Later, Njoku and Imani listened to a message from a woman in Florida. A child could be heard crying in the background; the caller’s voice sounded small and panicked. When Njoku called her back, the woman told her that she was in her early twenties, with two children, and that she was on Medicaid, unemployed, and eight weeks pregnant. Her abortion, scheduled for the next day, would cost nearly six hundred dollars, and she had only a little more than two hundred. Njoku asked what she had been doing to raise more money. The woman was thinking of pawning her wedding ring. “Oh, goodness, I don’t want you to have to do that,” Njoku said. “Hold on to that. We’ll figure it out before it has to get to that point.”