Pregnancy as an “inconvenience”
One of the greatest falsehoods of the pro-life movement is that pregnancy is merely an inconvenience, a period of temporary discomfort. This is more than a mere talking point; it’s a dangerous lie. Pregnancy is actually a life-threatening condition for many women.
The maternal mortality rate (MMR) is significantly higher in the US than in other developed countries, and the number gets even more pronounced when divvied up into demographics. The 2010 MMR in the US was 21 maternal deaths out of 100,000 live births, a number higher than 47 other countries listed by the CIA’s WorldFact report on maternal mortality. Compare this to the US Dept. of Health and Human Services’ goal for 2010 of 3.3 deaths per 100,000, and about seven times as many women are currently dying from pregnancy-related causes in the US than should be.
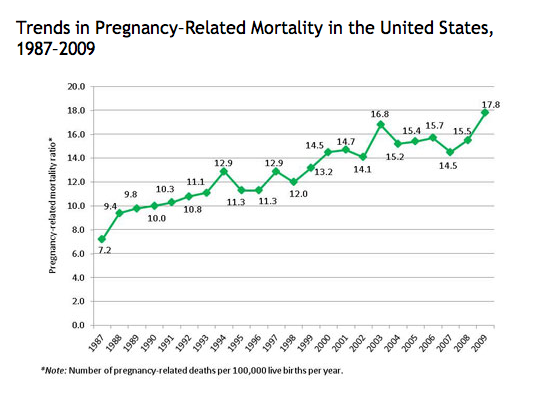
Shockingly, not only has the maternal mortality rate not fallen since the mid-1980s, it has actually steadily risen (the MMR in 1987 was 6.6!). But racial disparities in the MMR reveal even more appalling numbers: in 2007, black women were 2.7 times more likely to die of pregnancy-related causes than white women. A 2005 paper on the preventability of pregnancy-caused deaths in North Carolina showed that while 33% of deaths among white women were preventable, a full 46% of deaths among black women were preventable. This is probably reflective of wider disparities: minority women are more likely to experience an unintended pregnancy, to be poor, and to receive care at lower quality medical centers than white women.
Even worse, most of these figures are likely underestimated. A 2005 study compared actual rates of pregnancy-caused death to purported rates on death certificates in four regions and found a prevalent underestimation of pregnancy as a cause of death. In Massachusetts, death was inaccurately accorded to a cause other than pregnancy in 93% of the cases studied.
While the maternal mortality rate is increasing, the rate of severe pregnancy complications is also increasing. A 2009 study analyzing trends in the rates of severe obstetric complications showed a “20% increase in rates of renal failure, respiratory distress syndrome, shock, ventilation, and an approximately 50% and 90% increase in pulmonary embolism and blood transfusions, respectively” from 1998-2005. Although there was a correlation between increasing rates of (often unnecessary) caesarian section and severe complications, this only partially explained the dramatic rise in severe obstetric problems experienced by American women since 1998.
In addition, the infant mortality rate is also relatively high in the US compared to other developed countries. Despite substantial decline over the course of the 20th century, the rate of infant death has stagnated in recent years and the US international ranking for infant mortality fell from 12th place in 1960 to 30th in 2005. Abysmally, a Save the Children report recently showed that the US has the highest first day infant death rate of all industrialized nations studied in the report, 50% more than all other industrialized nations combined. And, as with the maternal mortality rate, racial disparities in the infant mortality rate are stark: according to the National Vital Statistics Reports for 2009, the mortality rate for black infants was 12.71per 1,000 live births, compared to 5.32 for white infants (and the report noted that the former is likely an underestimation).
And yet, as part of so-called “informed consent,” pro-life groups routinely tout the fallacious risks of abortion with pseudoscientific claims (e.g. increased risk of breast cancer, infertility, depression, and death) while understating the risks of childbirth. Among first trimester abortions, which comprise the vast majority of abortions, the risk of serious complications is less than .5%. However, more than 50,000 women per year suffer from severe maternal morbidity (SMM), potentially life-threatening conditions associated with pregnancy. The rate of SMM is also increasing over time, more than doubling from 1998 to 2011. This does not include more minor complications, which are far more common in pregnancy (94.1% of the pregnancies in 2008) than first trimester abortion (2.5%).

What should we be doing?
First, and perhaps most importantly, we need to gather information. Why, besides increased caesarian sections, are the rates of severe obstetric complications increasing? Why is the maternal mortality rate increasing so steadily despite the $86 billion spent on pregnancy and childbirth in the US per year? How can we standardize data collection to ensure accurate information on maternal health outcomes across the board? What programs can hospitals institute to reduce the rate of mortality for women and infants?
Although we have some notion of risks associated with maternal and infant death, our data is far from complete. In 2011 the Maternal Health Accountability Act was introduced to provide grants to create state-level maternal mortality review committees to standardize data collection and eliminate disparities in health outcomes. The bill unfortunately died in a Republican-controlled committee.
Otherwise, we are aware of many of the risks and should be able to address at least some with public policy. Higher risk of infant mortality is associated with preterm birth, which is associated with teen pregnancy, unplanned pregnancy, and poor/minority mothers.
These risk factors overlap significantly; for instance, teen mothers are more likely to be poorer, less educated, and to receive less prenatal care than mothers in other groups, and 70% surveyed in a 2004-2006 North Carolina study indicated that their pregnancies were unintended. Similarly, poor and minority women are less likely to receive prenatal care, and minority women are more likely to be poor and have higher rates of unintended pregnancy than other women as well. As for maternal mortality, disparities in access to prenatal and labor care and family planning; poverty; and minority status are all major risk factors, and these also often overlap.
While the problem is systemic, it can be tackled in very specific ways. One of the most important steps in tackling poor health outcomes for mothers and infants is to reduce unplanned pregnancy, which is indirectly associated with both infant and maternal mortality, since the groups at highest risk of dying of pregnancy complications and/or losing an infant are also at very high risk of unintended pregnancies. The major means of accomplishing this goal are to offer comprehensive sex education to adolescents, to increase public funding to family planning clinics, and to make access to reliable contraceptives as universal as possible.
Every one of these things has been directly evidenced to reduce the rate of unintended pregnancy. Comprehensive sex education is associated with reduced rates of teen pregnancy. Conversely, abstinence-only education has not been correlated with lower rates of vaginal intercourse, and states with abstinence-only or non-requisite sex education programs consistently have some of the highest rates of teen pregnancy in the nation. But that doesn’t stop pro-life politicians from routinely insisting on abstinence-only programs, despite their marked failure year after year.

For six in ten patients using publicly funded family planning services, it is their primary source of health care. An estimated 1.94 million unintended pregnancies and 810,000 abortions are prevented each year by use of public family planning clinics, but as I noted in my last article, they only meet a paltry 40% of the need. Increasing funding to family planning clinics, and therefore access to preventive services and contraceptives, would further decrease the rate of unplanned pregnancy. However, Republican politicians in numerous states consistently cut funding to family planning and women’s health services.
To give an example of the cognitive dissonance so prevalently present between stated pro-life ideology and the consequences of implementing pro-life laws, let us take Texas for an example. In 2011, as part of a sweeping pro-life agenda to shut down Planned Parenthood (the ultimate abortion scapegoat, despite 97% of its services being non-abortion related), Texas slashed family planning funds by 2/3 and barred Planned Parenthood from receiving funds from the Texas Women’s Health Program, resulting in a 77% reduction in the number of patients using family planning clinics, in a state that ranks first in the nation for the number of uninsured, 8th for poverty, and 3rd for teen pregnancy.
The maternal mortality rate has quadrupled in Texas in the last 15 years to 24.6, and even after improvement from 2009, the 2010 demographics are abysmal and much higher than the national average (27, down from 30.8, for white women, and 53.9, down from 66, for black women). For reference, that means black women are statistically better off giving birth in Mexico or Kazakhstan than Texas, and that white women would be better off in Saudi Arabia.
In addition, despite the incredibly high teen pregnancy rate, Texas schools stress abstinence education, do not require contraceptive education, and do not require that sex education be medically accurate. The budget cuts for women’s health care have also decreased the number of clinics that offer preventive healthcare for sexually active teens without parental consent or notification.
Every policy outlined above is one that increases the rate of unintended pregnancy, especially in populations more highly prone to infant mortality (teens) and maternal mortality (poor and minority women). Far from being “pro-life,” Texas has implemented a set of policies that will result in the unnecessary deaths of women and infants. It has instituted legislation that directly decreases access to contraceptives, preventive screenings, checkups, and prenatal care. These in turn lead to increased rates of poor health outcomes for pregnant women, as well as unintended pregnancy among the groups least likely to want or afford pregnancy or children. Simultaneously Texas has instituted sweeping anti-abortion policies that vastly remove access to abortion for women who can’t afford prenatal care or postpartum checkups.
The state ironically takes no responsibility for its own role in making women’s lives worse, exhibiting Orwellian double-speak about personal responsibility even as politicians systematically remove the resources women would otherwise use to BE personally responsible for their reproductive destinies.
All of Texas’ legislative actions aimed at shuttering the Planned Parenthoods in the state are particularly cruel considering they have also declined to expand Medicaid, leaving many poor and minority women nowhere to turn for contraceptives, preventive healthcare, and prenatal care. The Texas Policy Evaluation Project’s survey of low-income women following Texas’ 2011 budget cuts found that “now more than ever disadvantaged women must choose between contraception and meeting other immediate economic needs.”
Texas, sadly, is not alone. Many other states are likewise instituting anti-abortion restrictions while failing to address the unmet need for family planning, expand Medicaid, increase access to prenatal and postpartum care, or offer comprehensive or medically accurate sex education. Far from being an “inconvenience,” pregnancy is a condition fraught with major risks of health complications for both mother and infant. And when legislators intentionally limit abortion access while failing to address the increased risks of maternal and infant death that accompany high unintended pregnancy in poor, uneducated, teen, and minority women, they really don’t deserve to be called “pro-life.”
Sources:
1) “Deadly Delivery: The Maternal Health Care Crisis in the USA.” Amnesty International. http://www.amnestyusa.org/sites/default/files/pdfs/deadlydelivery.pdf
2) Berg CJ, Harper MA, et al. Preventability of pregnancy-related deaths: results of a state-wide review. http://www.ncbi.nlm.nih.gov/pubmed/16319245
3) Hasnain-Wynia R, Baker DW et al. Disparities in health care are driven by where minority patients seek care: examination of the hospital quality alliance measures. http://www.ncbi.nlm.nih.gov/pubmed/17592095
4) MacDorman MF, Mathews, TJ. The Challenge of Infant Mortality: Have We Reached a Plateau? http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2728659/
5) “Surviving the First Day: State of the World’s Mothers 2013”. Save the Children: http://www.savethechildrenweb.org/SOWM-2013/files/assets/common/downloads/State%20of%20the%20WorldOWM-2013.pdf
6) CIA World Factbook rankings of countries by maternal mortality rate: https://www.cia.gov/library/publications/the-world-factbook/rankorder/2223rank.html
7) Kochanek, K., Xu, J., et al. Deaths: Preliminary Data for 2009; National Vital Statistics Reports. http://www.cdc.gov/nchs/data/nvsr/nvsr59/nvsr59_04.pdf
8) Xu, J., Kenneth, D., et al. Deaths: Final Data for 2007; National Vital Statistics Reports. http://www.cdc.gov/nchs/data/nvsr/nvsr58/nvsr58_19.pdf
9) Gaskin, Ina. Maternal Death in the United States: A Problem Solved or a Problem Ignored? Journal of Perinatal Education, 2008. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2409165/#citeref9
10) Deneux-Tharaux, C, Berg, C, et al. Underreporting of Pregnancy-Related Mortality in the United States and Europe. 2005: http://opac.invs.sante.fr/doc_num.php?explnum_id=4060
11) CDC fact sheet on Severe Maternal Morbidity in the US: http://www.cdc.gov/reproductivehealth/MaternalInfantHealth/SevereMaternalMorbidity.html
12) National Abortion Federation fact sheet on the risks of abortion: https://www.prochoice.org/about_abortion/facts/safety_of_abortion.html#n5
13) Elixhauser A, Wier M. Complicating Conditions of Pregnancy and Childbirth, 2008. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb113.pdf
14) “Unintended Pregnancies: 2004-2006 N.C. Pregnancy Risk Assessment Monitoring System (PRAMS)” http://digital.ncdcr.gov/cdm/ref/collection/p249901coll22/id/22589
15) An epidemiological review of the effects of comprehensive, abstinence-only, and lack of sexual education on the likelihood of teen pregnancy and rate of intercourse: http://www.jahonline.org/article/S1054-139X(07)00426-0/abstract
16) Teen pregnancy rates by state: http://www.livescience.com/27417-teen-pregnancy-rates-by-state.html AND, for comparison, a brief on state policies on sex education: https://www.guttmacher.org/statecenter/spibs/spib_SE.pdf
17) Guttmacher news release on unintended pregnancies and abortions prevented by the use of publicly funded family planning services: https://guttmacher.org/media/nr/2009/02/23/index.html
18) 77% fewer Texas clients for family planning clinics: http://rhrealitycheck.org/article/2013/11/21/after-budget-cuts-texas-family-planning-program-serving-77-percent-fewer-clients/
19) Texas has highest uninsured rate and ranks 8th for poverty: http://dfw.cbslocal.com/2013/09/17/texas-has-highest-uninsured-rate-high-poverty/
20) “Republicans Offer an Obamacare Alternative,” Time Healthcare online: http://swampland.time.com/2014/02/03/obamacare-republican-alternative/
21) The Texas Policy Evaluation Project, “Low-Income Women’s Attitudes About Affordable Family Planning Services” http://www.utexas.edu/cola/orgs/txpep/_files/pdf/TxPEP-ResearchBrief-WomensAttitudesAboutFPServices.pdf