In an interview published in The Hill, Democratic campaign chairman Ben Ray Luján said that the party would financially support candidates who oppose abortion. The primary rationale for opening up the party’s base to anti-abortion candidates is to win House majority in 2018. In addition to that, Luján said that there was no “litmus test” for Democratic candidates. The Democratic Congressional Campaign Committee chairman justified the move by saying that the party needed candidates to “fit” their respective districts in order to score victory.
“There is not a litmus test for Democratic candidates,” Luján explained, “As we look at candidates across the country, you need to make sure you have candidates that fit the district, that can win in these districts across America.”
The Hill noted that Luján had been working on gaining more candidates in order to defeat Republicans in the 2018 midterm elections. The chairman put emphasis on having a “big [Democratic] family” to win House majority in 2018. He said, “To pick up 24 [seats] and get to 218, that is the job. We will need a broad coalition to get that done.”
Luján isn’t the only prominent Democrat against litmus tests for Democratic candidates. Prior to him, House Minority leader Nancy Pelosi and Senate Majority leader Charles Schumer have criticized and opposed party litmus tests.
In spite of Luján’s reasoning for casting a wide and diverse net for Democratic candidates, some believe that the party’s decision will end up alienating those who support free choice, abortion, and fair reproductive health care. People like Mitchell Stille of NARAL Pro-Choice America criticized the move and said that supporting anti-abortion candidates was “bad politics that will lead to worse policy.”
Even within the party, there are those who would disagree with Luján’s position. Chair of the Democratic National Committee Tom Perez would be one of them. Back in April, Perez noted that abortion and reproductive health care were critical issues for Democrats.
In a statement to the public, Perez shared his thoughts and said, “Every Democrat, like every American, should support a woman’s right to make her own choices about her body and her health. That is not negotiable and should not change city by city or state by state.”
PRO-CHOICE CAMPAIGNERS AT A NATIONAL MARCH FOR WOMEN’S LIVES IN WASHINGTON DC, 9TH MARCH 1986. (PHOTO BY BARBARA ALPER/GETTY IMAGES)
PHOTO: BARBARA ALPER
It’s no secret that President Donald Trump, his administration, and Republican lawmakers are trying to dismantle women’s reproductive rights in 2017. Trump has already taken steps to defund Planned Parenthood and expand the global gag rule. The Department of Health and Human Services hired women who have said that contraception doesn’t work, that IUDs have “life-ending properties,” and that abstinence-only education works to serve in leadership positions. Republicans in Congress are trying to dismantle health care provided to women by the Affordable Care Act. The list goes on and on, but this is not the time to give up.
Despite the threats to reproductive rights at the federal level, state legislators are finding ways to protect women. States have always been vital to expanding and restricting reproductive rights. Before Roe v. Wade in 1973, for example, states decided the legality of abortion, and only three had repealed their abortion lawsby the time the landmark decision was made. But while Roe v. Wade took away one decision for states, according to Gloria Totten, the founder and president of a policy and leadership center called the Public Leadership Institute (PLI), plenty of other legislation that threatens women—attacks on Planned Parenthood, shutting down abortion clinics, and enacting bans on specific procedures—often starts at the state level. However, the reverse is true too, and state lawmakers are harnessing their power to enact policies that protect and expand women’s reproductive health rights.
For example, New Mexico just approved a new policy whereby pharmacists can directly prescribe women birth control, a move officials say will help women in the largely rural state have better access to contraception. Democratic lawmakers in Nevada are working to pass a bill that would require all insurers to cover patients’ contraception, regardless of a business owner’s religion. They also just passed legislation to make insurers cover 12 months of birth control at a time without copayments; Colorado recently signed a similar bill into law, and Virginia has one in the works.
With abortion rights threatened by a Supreme Court dominated by conservatives, it’s state lawmakers who will have to step up if Roe v. Wade is dismantled. The state of Maryland just enacted legislation to guarantee Planned Parenthood funding in the event that the federal government cuts it. Oregon is looking to pass a law that would require all insurers to cover abortions in the state regardless of a person’s gender, income, or citizenship status. Meanwhile, Illinois is trying to undo a “trigger law” that would outlaw and criminalize abortion if the Supreme Court’s historic Roe v. Wade decision was ever overturned, and New York Governor Andrew Cuomo has proposed writing a woman’s right to an abortion into the state constitution—a major achievement for a state whose biggest city has been called “The Abortion Capital of America” for its centuries-old progressive views on the issue.
But there’s a long way to go before every state actually respects reproductive rights. Each of these bills faces resistance from antiabortion activists, but tensions between community activists and lawmakers who are trying to pass actual reproductive rights legislation can be just as damaging to the process.
“Part of the advice that we’re constantly giving both the lawmakers and the advocates is that you need to start working together early on in the process,” Totten tells Glamour. Totten’s organization offers support to local and state-level lawmakers, providing resources to better understand the issues and figure out the best tactics for passing legislation. “Too often what we find is that policymakers will say, ‘I want to do something!’ and they’ll know their legislative process really well. Or the advocates will say they want to do something and they’ll know the external environment really well, but [lawmakers and advocates] fully bake their ideas before coming together,” Totten notes.
One of PLI’s recent achievements was convincing 52 lawmakers across 27 different states to pledge to introduce proactive abortion rights legislation. Totten hopes lawmakers will meet with advocates and organizers earlier in the process of drafting legislation to streamline the system and figure out how to effectively promote and enact bills.
For those looking to get involved in reproductive rights issues close to home, Totten says people should look for nearby chapters or affiliates of organizations like Planned Parenthood, NARAL, and interfaith alliances, many of whom also work with legislators.
Even with these encouraging developments, Totten knows not every proabortion bill will get passed—in many cases, they won’t even be debated, let alone get a vote. But that doesn’t mean it’s time to throw in the towel. “In most places we will not pass anything, so we have to be even more strategic about when we’re using policy,” she says. The fight might seem overwhelming at times, but Totten knows from experience that even the smallest actions—like getting groups to sign resolutions or volunteering with proabortion organizations—really do add up.
People hold signs as they attend an anti-abortion rally at the Arkansas state Capitol in Little Rock, Ark., Sunday, Jan. 18, 2015.
LITTLE ROCK, Ark. — A federal judge has blocked Arkansas from enforcing four new abortion restrictions, including a ban on a common second trimester procedure and a fetal remains law that opponents say would effectively require a partner’s consent before a woman could get an abortion.
U.S. District Court Judge Kristine Baker issued a preliminary injunction late Friday night against the new restrictions, three of which were set to take effect Tuesday. The American Civil Liberties Union and the Center for Reproductive Rights had challenged the measures, suing on behalf of Dr. Frederick Hopkins, a Little Rock abortion provider.
The laws include a ban on a procedure known as dilation and evacuation. Abortion-rights supporters contend it’s the safest and most common procedure used in second-trimester abortions. Similar bans are in effect in Mississippi and West Virginia and have been blocked by court rulings in Alabama, Kansas, Louisiana and Oklahoma. A ban approved in Texas will take effect in September and is also being challenged in court. The groups said the ban would have a devastating impact, while the state argued that alternative procedures are available.
“The threatened harm to Dr. Hopkins and the fraction of women for whom the Mandate is relevant clearly outweighs whatever damage or harm a proposed injunction may cause the State of Arkansas,” Baker wrote in her ruling.
The attorney general’s office did not have an immediate comment on the ruling. Attorneys for the ACLU of Arkansas did not immediately reply to messages early Saturday morning.
Baker’s ruling also halts a law that would impose new restrictions on the disposal of fetal tissue from abortions. The plaintiffs argued that it could also block access by requiring notification of a third party, such as the woman’s sexual partner or her parents, to determine what happens to the fetal remains. The state has said the law doesn’t require permission or notice from those third parties before an abortion and includes several provisions that ensure notice or consent isn’t required to dispose of the fetal remains.
Baker said the disposal law’s requirements would dissuade doctors from performing abortions and create significant delays for women seeking the procedure.
“For these reasons, the Court is not convinced that importing the (disposal law’s) complex requirements for authorization advances a public health goal,” Baker wrote. “These requirements also do not advance interests in women’s health because delay and other negative effects instead threaten women’s health and wellbeing.”
Baker also blocked part of a law set to take effect in January that would ban abortions based solely on the fetus’ sex. The groups are challenging the law’s requirement that a doctor performing the abortion first request records related to the entire pregnancy history of the woman. The plaintiffs say the requirement would violate a patient’s privacy and indefinitely delay a woman’s access to abortion.
The judge also blocked a law that would expand a requirement that physicians performing abortions for patients under 14 take certain steps to preserve embryonic or fetal tissue and notify police where the minor resides. The new measure, which was also set to take effect Tuesday, would have raised the age requirement to less than 17 years of age.
The ruling came hours after a federal appeals court panel cleared the way for Arkansas to enforce a law that will limit how the abortion pill can be administered. The panel lifted Baker’s order blocking the 2015 law requiring doctors who provide such pills to maintain a contract with another physician who has admitting privileges at a hospital and who agrees to handle any complications. The state can’t enforce the abortion pill restrictions until the appeals panel’s ruling takes effect in about two or three weeks.
On the ground during one of the most trying times for the pro-choice movement.
LOUISVILLE, KENTUCKY — It’s 6:15 in the morning and 30 people are already standing outside the E.M.W. Women’s Surgical Center in Louisville, Kentucky, the last operating abortion clinic in the state. The center doesn’t open for another two hours, but the fight for space in front of the clinic starts early.
Protesters praying in front of the E.M.W. clinic in Louisville, KY CREDIT: Katelyn Marmon
About half of the people here are anti-abortion activists, setting up three speakers, a microphone and a sound board as well as unpacking a stack of huge poster boards. Next to them are the Louisville Clinic Escorts, men and women who volunteer to escort patients from their cars into the clinic. They wear purple vests with “clinic escort” written on the front and back so the patient can identify them. And standing on the outskirts of the sidewalk are U.S. Marshals as well as Louisville metropolitan police. The marshals are here for the week to enforce a temporary buffer zone that keeps the seven feet of sidewalk in front of the clinic’s doors unoccupied; a necessity after 10 protesters were arrested in May for blockading the doors to the clinic.
The sun hasn’t come up yet, but the protesters have already begun their work. Christian music, preaching, and prayers stream through the speakers, which are turned toward the clinic’s waiting room for the patients and staff to hear.
CREDIT: Katelyn Marmon
“This is a real evil, and it’s really about exposing that evil,” said John Pride, a member of Operation Save America, a fundamentalist Christian group that organized a national protest of the EMW clinic this week in Kentucky.
For the first hour, only men are among the protesters. They scroll through the available posters, picking their favorite and holding it up to face the oncoming traffic. The posters feature graphic photographs of aborted fetuses and text like “Never forget that everything Hitler did in Germany was legal.”
As for the escorts — they wait. Their jobs are not to engage, not to counter protest, and not to even look at the protesters if they can help it. They stand along the property line of the clinic as well as station themselves in the parking lot to help direct patients where to go.
A clinic escort stands along the buffer zone as a protester prays over her. CREDIT: Katelyn Marmon
This job has gotten harder in the last few years, after a Christian “crisis pregnancy center” — an anti-choice organization focused on dissuading patients from going through with an abortion — bought the building right next door to the clinic. The pregnancy center employees will try to direct the women into their office before they have a chance to get to the clinic; they even offer free parking for patients who have an appointment at the E.M.W. Women’s Surgical Center but choose to come to the pregnancy center instead.
Clinic escorts wait along the property line for patients to arrive as protesters try to engage them in conversation. CREDIT: Katelyn Marmon
On this morning, some protesters try to engage the escorts, either by standing directly in front of them and talking to them or by shouting into the microphone. Others pray over the escorts while standing next to them. Some don’t engage at all but stood to the side of the entrance, silently praying the rosary while wearing oversized “Choose Life” t-shirts.
“It’s very much an assault,” said Sarah Dugan, an escort who was stationed next to the the speakers. “But you get really good at ignoring it.”
As the sun starts to rise, a cargo truck drives by the clinic, all sides of its trailer covered in the same graphic anti-abortion images as the protesters’ posters. The truck circles the block for the next several hours.
By this point there are at least 60 people gathered around the still unopened clinic. Twenty officers have shown up along with 21 escorts. As each minute passes, more protesters arrive on the scene, bringing more posters, pamphlets, and a baby’s coffin with children’s toys and two fetus figurines.
At 8:00 a.m, a bell rings to signify that the clinic is open. So far, only one patient has been brought in and she was able to enter the clinic unnoticed so the protesters weren’t able to confront her in person.
A protester shouts through the window at the patient inside the E.M.W clinic CREDIT: Katelyn Marmon
After seeing a hand peek through the waiting room, two protesters attempt to directly engage with the patient through the window. “Young lady, having your baby murdered this morning is not loving,” the protester shouted through cupped hands towards the drawn blinds in the waiting room.
Patients only arrive for the first 30 minutes after the clinic opens, so by half past 8 a.m., the escorts’ jobs are done. They quietly take off their vests and disperse — some to eat breakfast together and decompress, and some to go straight to work. The protesters, on the other hand, have set up folding chairs and tables. For them, the job is far from over.
Despite the federal government’s sustained plan to thwart women’s reproductive freedom, a new mid-year report from the National Institute for Reproductive Health (NIRH) reveals a welcome trend; since January, 49 states have introduced almost 600 pieces of legislation to protect and advance access to reproductive health care services.
NIRH President Andrea Miller points to positive and proactive developments even in states like Nevada and Maine, both led by Republican governors. Each has passed laws that mandate insurance companies cover the cost of all FDA-approved contraception. And in state governments under Democratic control, like Maryland, for example, bills have been introduced that would pony up state funds to support Planned Parenthood if the federal government defunds it.
“We’re in a moment where we know the federal government is working to overturn Roe v. Wade, to dismantle access to affordable health care, to defund Planned Parenthood, to reverse the no-copay for contraception [essential health care benefit], to deny family planning funds to clinics that provide abortions,” Miller says. “And yet, we have seen that states are…taking action to really counter that devastating trend at the national level.”
Of course, that’s not to suggest that states haven’t passed their fair share of anti-choice legislation. According to The Huffington Post, Arizona, Arkansas, Florida, Indiana, Kansas, Louisiana, Mississippi, Oklahoma, and Texas have all tried to deny Planned Parenthood government dollars. And Miller acknowledges that at least 379 anti-choice laws have passed in the United States since 2010. “But nonetheless,” she’s been heartened to see some states take steps to ensure if not access to abortion, then at least access to family planning and contraceptive services. “There is incredible opportunity,” Miller continues. “And we’re seeing advocates and policymakers at the state level really declare that enough is enough: ‘We are not going to stand by and let the federal government dictate women’s decisions. We are going to step into that breach and take care of our residents.'”
These women do not represent some niche statistic. And it does states no favors to dismiss their needs. The Guttmacher Institute estimates that at least 38 million women seek contraception because they’re sexually active and don’t want to be pregnant. And no matter what Secretary of Health and Human Services Secretary Tom Price suggested, they can’t all afford contraception. In 2014, a full 20 million of these 38 million women needed publicly funded services because their income fell below 250 percent of the federal poverty level or they were under 20 years old. Guttmacher found that publicly funded family planning services from all sources in 2014 helped women avoid roughly two million unintended pregnancies; had they not had that access, the organization estimates that nearly one million women would have carried unintentional pregnancies to term and almost 700,000 would have had abortions.
“It’s essential that we push back against the attacks coming Washington, D.C.,” Miller says. “But it’s as important to make sure that people are reaching out to their elected officials at the state level and in their municipalities, because those are the people who have a direct and immediate opportunity to influence access to reproductive health care in communities nationwide.”
The latest NIRH research has determined that 80 bills or pieces of legislation were proposed in 26 states to ensure women be able to access abortion. Already, four states have implemented them—Delaware, Idaho, Illinois, and Oregon. “In terms of access to contraception services,” Miller says, “more than 90 bills were introduced, and six states and the District of Columbia have enacted some version of them that will improve access to contraception for residents.”
“When women and young people have access to reproductive health services, everyone thrives,” Miller says. “It means fewer unintended pregnancies and more women who can determine for themselves when they want to have children. It means that you’re not having to deal with these problems after the fact because you’ve denied people access to services that so fundamentally affect whether they can make decisions that shape their lives.”
The first six months of the Trump administration have witnessed the expansion of the global gag rule, which withholds U.S. dollars from health care providers around the world that so much as mention the word “abortion,” the rollback of Obama-era protections for Planned Parenthood, the leak of a rule that could, if implemented, deny hundreds of thousands of women access to birth control, and the rise of men like Price.
The moves have certainly had a trickle-down effect, empowering anti-choice politicians in states like Texas and Iowa to take unprecedented steps to defund Planned Parenthood, close clinics, and attempt to ban some of the safest abortion procedures available to women. But they’ve inspired a resistance at the state level that the new NIRH proves. 600 pieces of good news are nice, but proposed legislation is not enough. So the next time you can’t get through to your senators, dial your state representative. Make sure they know you have a uterus, and you vote.
“At a time when young people are most in need of information and education to protect their sexual and reproductive health, this administration is denying evidence and science.”
A letter from members of Congress called the Trump administration’s decision “a blow to bipartisan efforts to prevent unplanned teen pregnancies.” Shutterstock
A letter issued Tuesday from 148 members of Congress to Health and Human Services (HHS) Secretary Tom Price demands an explanation for why the Trump administration ended grants for some teen pregnancy prevention programs.
The letter called the Trump administration’s decision “a blow to bipartisan efforts to prevent unplanned teen pregnancies.” It comes after the Center for Investigative Reporting’s Revealreported this month that HHS had “quietly axed $213.6 million in teen pregnancy prevention programs and research at more than 80 institutions around the country.”
According to the letter, HHS will “shorten the project period for Office of Adolescent Health’s (OAH) Teen Pregnancy Program from five years to three years.”
“The negative impacts of this unnecessary decision cannot be overstated,” the letter continues. “At a time when young people are most in need of information and education to protect their sexual and reproductive health, this administration is denying evidence and science.”
“Young people deserve better,” it said.
The letter asked for Price to explain who made the decision to cut the program, when that decision was made, and how the decision factored in “the burden and adverse impact for young people being served, the professionals and partnerships, and their communities.”
Rep. Barbara Lee (D-CA) said in a statement that she is “appalled that this administration would abandon the young people who rely on this program to stay healthy.” “This irresponsible decision leaves youth without the information and skills they need to make safe and healthy choices,” she said, adding that “Price must provide an explanation for this egregious action and work with Congress to rectify it immediately.”
Dr. Willie Parker, one of Alabama’s few remaining abortion providers, works in the Huntsville clinic. (Chloe Angyal/HuffPost)
More
HUNTSVILLE, ALABAMA — Dr. Willie Parker, one of Alabama’s few remaining abortion providers, was driving to work when he got the call. The name “Dalton Johnson” flashed on the SUV’s dashboard screen, as Parker switched on his headset. He listened as Johnson, the owner of the abortion clinic where he was headed, explained the problem.
A patient at the Huntsville clinic who was 21 weeks pregnant needed an abortion, but she was also a regular user of opioids. This meant she wouldn’t be able to receive medication to help ease the pain of the procedure ― which, like any surgery, can be agonizing ― because her use of opioids could nullify the effects of many pain relievers.
After about 15 minutes of discussion, Parker told Johnson he couldn’t take the case. “I hate to turn anyone away,” he said after hanging up. “But if something goes wrong, no one is going to remember that I was trying to help this woman.”
Alabama, like the rest of the nation, has been hit hard by the opioid crisis, with overdose deaths at an all-time high and a generation of children making their way into foster care. But other victims of the crisis ― victims who are not uncommon ― are pregnant women seeking abortions, like the patient at the Alabama Women’s Center for Reproductive Alternatives in Huntsville.
Parker says these women tend to be poor, white and in their second trimester. It’s not that they wait until the last minute to seek an abortion, he added. It’s more a matter of not knowing they’re pregnant ― opioid users may ovulate less frequently and therefore have irregular cycles ― and not having enough money to pay for an abortion.
“Their lives may not be together enough to get in early to get the abortion,” he said. “When they show up and they’re 15 or 16 weeks, they say they didn’t know they were pregnant.” He added that most of the women he sees are African-American, but of the opioid-addicted women he treats, most of those patients are white.
Abortion providers say they are seeing an uptick in pregnant women who fit this profile. Johnson estimates about 10 percent of patients use opioids.
Gloria Gray, who runs the West Alabama Women’s Center in Tuscaloosa, has seen a similar uptick. “It’s very unfortunate, because there’s not much we can do to help them,” she said. “We could give them everything we have in the clinic and it wouldn’t faze them.”
Gray said her nurses are now having to discourage opioid-addicted patients from self-medicating in preparation for the procedure. “We just have to talk to them and explain it to them that they’re going to have to have a strong will and a strong mind,” she said, adding the nurses try to be upfront with the women, but “those are the ones that usually end up screaming.”
Gloria Gray, owner of the West Alabama Women’s Center, stands outside her Tuscaloosa clinic. (Chloe Angyal/HuffPost)
More
Alabama leads the nation in its ratio of opioid prescriptions per capita, at 1.2 prescriptions per person compared with the national average of 0.76. Its increase in opioid deaths between 2014 and 2015 was one of the five greatest in the nation, and the state attorney general says Alabama has “disproportionately suffered” from the opioid epidemic.
Alabama also has some of the nation’s most severe restrictions on abortion. To obtain an abortion at one of Alabama’s four remaining clinics, a woman must make two trips to the clinic, 48 hours apart. The first visit involves an ultrasound during which the provider must offer the patient the option to view the image. It also involves state-mandated “counseling” which, like the state-mandated brochures clinics are required to offer patients, is designed to discourage abortion. (One brochure refers to the fetus as “the unborn child.”)
Even patients who are obtaining the abortion pill, which induces a miscarriage that happens off the premises, are required to make two appointments.
The state’s legal cutoff for abortion is 22 weeks, making it a destination for women from states with more stringent cutoffs; at Johnson’s clinic and at the clinic in Tuscaloosa, where Parker also practices, patients come from Tennessee, Florida and Mississippi.
Dalton Johnson, who owns the Huntsville clinic, takes a call from a prospective client and explains the state’s waiting period laws. (Chloe Angyal/HuffPost)
More
Although the patient Parker and Johnson were talking about was from Birmingham, she was 21 weeks and 1 day pregnant, which meant her procedure would have to be a dilation and evacuation, or D&E. Parker would have to use drugs to soften her cervix to conduct the abortion procedure in order to be able to insert his instruments into her uterus and remove the fetus.
Softening (or “ripening”) the cervix ― which opens it up to allow for the abortion procedure to take place ― causes cramping and can take all day. Usually Parker would begin the softening process the day before the procedure. But this patient had come in on the Friday before the long Independence Day weekend.
The clinic wouldn’t be open again until the following Wednesday, by which point she would be perilously close to the 22-week cutoff. After that, her options would be so limited as to be meaningless: It’s possible to get an abortion after 22 weeks in the United States, but only in a few states, none near Alabama. The procedure would cost between $8,000 and $10,000 — and that’s before airfare, accommodation and days of missed work.
To add to the patient’s concerns, Alabama has been aggressive about prosecuting women who use drugs while pregnant. Given the abortion restrictions in surrounding states, given the looming public holiday and given this woman’s desire not to become a mother, Parker and Johnson both knew they were her last best hope.
None of these clinical challenges would be insurmountable for Parker under normal circumstances, but the patient’s drug misuse made the procedure complicated and was the reason Parker initially believed he could not help her.
Parker prepares to see his next patient. (Chloe Angyal/HuffPost)
More
The patient, who allowed a reporter from HuffPost to observe the process, refused to specify which drugs she had been using, saying only that she took “pain meds for anxiety.” Parker was worried that even the maximum pain relief he was permitted to give her at the clinic wouldn’t make a dent in the pain of the surgery, making the procedure unbearable for her.
The patient, 25, was petite ― about 115 pounds ― and had never given birth before, meaning her cervix was much tighter than it would have been had she already had a child. Pain relief would be required, but her opioid habit could render it ineffective. Unlike most opioid-using patients that Parker sees, this woman was African-American; most opioid users who come to the clinic are white, as that’s the population that’s been hit hardest in the area.
Opioids relieve pain by bonding to the body’s mu receptors, blocking them and thus their ability to convey pain. “The body isn’t dumb,” says Dr. Nitin Sekhri, a pain management specialist at Westchester Medical Center. “Once you start to block a receptor, it just makes more. So your body ends up with more pain receptors, and the pain relief treatment stops working.”
Moderate pain becomes extreme pain as the body makes more and more receptors in response to more and more opioids. This is opioid-induced hyperalgesia, and it’s an enormous challenge for doctors who need to operate on people who are addicted to opioids.
Parker said he wasn’t willing to take the risk of operating on someone whose pain might not be adequately controlled. It’s a clinical decision, but he also considered the political implications.
If something were to go wrong, the negative attention that would be trained on him and on the clinic, he said, could hinder their ability to provide abortions for other women.
Johnson says his clinic has performed about 20,000 abortions since 2001, and about eight of those cases have required hospitalization due to complications. Still, this case was close to the edge of Parker’s clinical abilities, and if something went awry, “it’s just another botched abortion,” he said, and a ripe opportunity for anti-abortion activists and legislators to pounce in the name of women’s health. As Parker explains in his recent book, Life’s Work: A Moral Argument for Choice, bending the rules and skirting the edge of his clinical abilities simply aren’t worth the risk.
In the end, Johnson and Parker agreed on a solution: Dr. Yashica Robinson, the clinic’s chief abortion provider, would do the patient’s procedure. Robinson is the only doctor other than Parker in Alabama performing abortions after 14 weeks. Robinson would perform a cervix ripening procedure using a transcervical Foley balloon, which Parker had observed but could not yet perform himself. Robinson inserted a catheter into the patient’s uterus and inflated it such that it put pressure on the cervix, causing dilation.
Dr. Yashica Robinson stepped in to perform a pre-abortion procedure to make the patient more comfortable during surgery. (Chloe Angyal/HuffPost)
More
Robinson waited until the very end of the day to perform the abortion, giving the patient’s cervix as long as possible to soften. The patient was lightly sedated and given non-opioid pain relief ― ibuprofen ― but the pain of the ripening process was considerable. At one point, she limped down the hall to the bathroom and begged for another pill as she’d vomited up the first one.
By the time Robinson put on her sterile shoe covers and a smock over her scrubs, the patient was drowsy, sedated and lying back on the chair with her feet in the stirrups.
The patient’s hair, cut in a bob and dyed green, was damp with sweat and disheveled after a day spent waiting in the clinic. Her T-shirt, white with hot pink writing, was pulled up to reveal her rounded belly and navel piercing.
Robinson verbally walked the patient through the procedure as she progressed through the stages, warning her when she might expect to feel pressure and when she might feel pain. The patient seemed to suffer less than Johnson and Parker expected, occasionally screwing up her face against the pressure, and just once saying, “ouch” at the pain. She was clearly not comfortable. But she wasn’t screaming.
The procedure took about 15 minutes, and in the end, the patient was surprised at its brevity. “Is it over?” she asked, looking up at Robinson as the doctor headed for the door. “Yep,” Robinson replied. “It’s over.”
Twenty minutes later, the patient walked into the waiting room with the help of a nurse. She was woozy and moving gingerly. She was certainly not fit to drive, but she had someone waiting there to take her home. It was a ninety minute drive home to Birmingham.
Johnson said that despite the possibility of enormous pain, most abortion patients who misuse opioids are “very determined” to obtain the procedure and to get through it. They’re “very motivated,” he said, noting that this patient had already been to another clinic, but was sent to Huntsville because she was so far along.
Parker changed out of his scrubs and got back in his car, nine hours and dozens of patients after Johnson’s call. “Like I said, I hate to turn anyone away,” he said, as he drove down the freeway in the gathering dark. On this day, they didn’t have to.
“There is no evidence that simply changing the Medicaid reimbursement threshold would sweep in any new providers, and it doesn’t change the fact that the provision itself is rooted in advancing a politically motivated social agenda.”
Protesters gathered July 24 to oppose Republican efforts to gut the Affordable Care Act.
Lauryn Gutierrez
Religious imposition laws are designed to shield private individuals and businesses from complying with nondiscrimination laws based on a religious objection to that service.
Senate Republicans are expected to vote Wednesday on a so-called “skinny” bill to repeal, but not replace, the Affordable Care Act (ACA), leaving millions without health insurance and lifting premiums by an estimated average of $1,238.
A copy of the bill circulating Wednesday would strip Planned Parenthood of Medicaid funds—with a new twist. The Senate bill prohibits Medicaid dollars from going to abortion providers that received more than $1 million in Medicaid reimbursements in fiscal year 2014. An earlier bill showed a dollar amount of $350 million.
It was unclear if Senate leadership changed the dollar figure in an attempt to skirt a Senate rule that nixed their plans to defund Planned Parenthood through the budget reconciliation process. Health policy advocates called the dollar change politically motivated.
“There is no evidence that simply changing the Medicaid reimbursement threshold would sweep in any new providers, and it doesn’t change the fact that the provision itself is rooted in advancing a politically motivated social agenda — the same reason why abortion policy provisions have always been determined to violate the Byrd Rule,” a health-care policy advocate told Rewire.
The Senate’s parliamentarian said last week that provisions like defunding Planned Parenthood violate the Byrd Rule and need at least 60 votes to pass.
The GOP bill includes eliminating tax credits to small employers with health-care plans that cover abortion care.
Wednesday’s vote represents Republicans’ latest attempt to strip vulnerable and low-income people of health-care coverage now that they control Congress and the White House.
Late Tuesday, Senate Republicans’ proposal to “repeal and replace” the ACA, or Obamacare, died by a wide margin. The “Better Care Reconciliation Act” would have dropped 15 million people from Medicaid and left nearly 50 million uninsured, according to the Congressional Budget Office, a nonpartisan legislative scorekeeper.
Early in the day, protesters disrupted the vote, with chants of “Kill the bill, don’t kill us!” and “Shame!” that could be heard in the Senate chambers.
Polls indicate the U.S. public greatly prefers Obamacare to various Republican alternatives that would take away health-care coverage from tens of millions.
Congressional Republicans have had seven years to come up with an alternative to Obamacare, but until now their legislation was consistently vetoed by former President Obama. Now, with President Trump tweeting he has his “pen in hand” ready to sign GOP legislation, Republicans are challenged to arrive at a consensus.
Even if the Senate manages to pass some form of Trumpcare, it would need approval by the House to become law.
As Washington moved to reduce federal funding for women’s health, the battle over affordable birth control and other women’s health services shifted to state capitals.
THE ASSOCIATED PRESS
Maryland House Speaker Michael Busch speaks at a news conference in Annapolis in support of legislation to protect funding for Planned Parenthood. Democratic lawmakers in Maryland and other states enacted a record number of laws in 2017 to protect women’s access to affordable birth control and other reproductive health services.
As Washington moved to reduce federal funding for women’s health this year, adversaries in the war over affordable birth control and other women’s health services shifted the battleground to state capitals — resulting in a spate of new laws that both expand and contract women’s access to care.
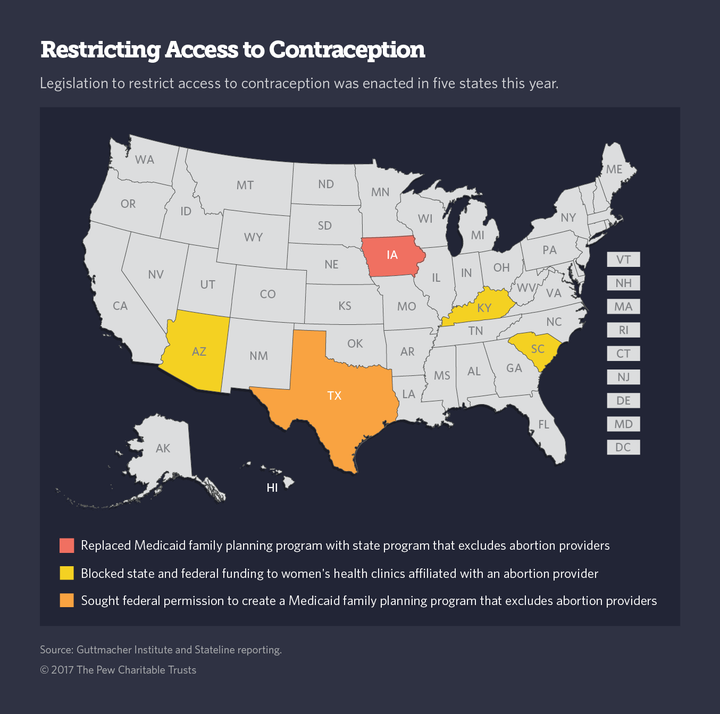
It happened quickly in Iowa. In May, then-Gov. Terry Branstad, a Republican, signed a bill defunding Planned Parenthood. Medicaid dollars stopped flowing to the group July 1, and four of the state’s Planned Parenthood clinics closed within a week.
That left nearly 15,000 women in small communities without access to reproductive health services, including cancer screenings, birth control, testing for and treatment of sexually transmitted diseases, and annual checkups.
Medicaid pays for three-quarters of all publicly supported women’s health programs. So when Iowa abruptly cut off Medicaid dollars to Planned Parenthood, it was game over, said Jodi Tomlonovik, executive director of the Family Planning Council of Iowa, which oversees distribution of federal and state money to women’s health clinics.
Iowa’s law, which applies to Planned Parenthood and any other women’s health clinics affiliated with a group that performs abortions, may also defund women’s clinics in the state’s largest health care system, UnityPoint Health, as well as the University of Iowa Hospitals and Clinics, because certain clinics in both groups perform abortions in cases of fetal abnormalities, she said.
In three other states with GOP governors and legislatures — Arizona, Kentucky and South Carolina — 2017 state budgets that exclude Planned Parenthood and other women’s health clinics affiliated with an abortion provider from all state and federal funding may have similar effects on local clinics.
And in a first-of-its-kind approach to defunding abortion providers, Texas asked the federal government in May for permission to recreate a Medicaid family planning program it eliminated four years ago so it could create a state-funded plan. This time, Texas wants to exclude Planned Parenthood and other abortion providers from participating in the program, and fund it with federal Medicaid dollars.
If the request is approved, many more states can be expected to file similar applications, said Elizabeth Nash, a policy analyst at the Guttmacher Institute, which tracks reproductive health policy.
Expanding Access
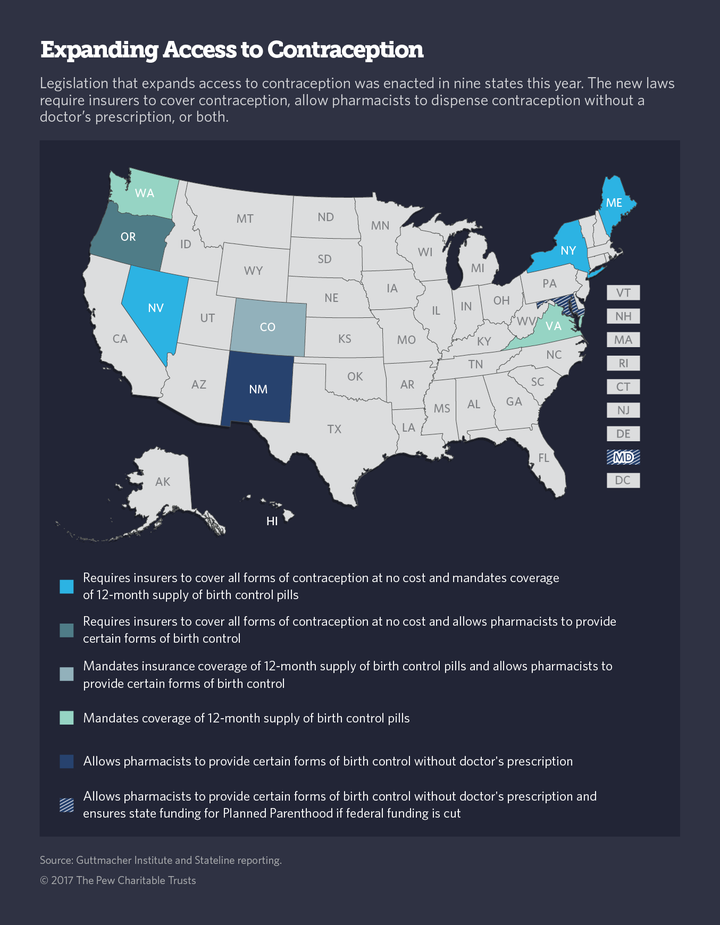
In sharp contrast, Nevada and Maine, both led by Republican governors, enacted new laws mandating insurance companies cover the costs of all U.S. Food and Drug Administration approved forms of contraception without delay and without requiring women to try the cheapest method first, as some insurers now do.
Oregon, a state with a Democratic governor and Legislature, did the same thing, adding abortions to the list of reproductive services insurers must cover. And Maryland became the first state to enact a law committing state funds to Planned Parenthood if federal funds are taken away.
Lawmakers in California, Connecticut, New Jersey, New York and Wisconsin considered similar measures this year. Nevada appropriated $1 million over two years for family planning services to replace any cuts in federal money for Planned Parenthood.
States also enacted two other types of laws designed to ease access to birth control pills and other forms of contraceptives. Colorado, Maine, Nevada, New York, Virginia and Washington enacted laws requiring all insurers to cover 12-month prescriptions of birth control pills to make it easier for women to take the pills without interruption, particularly those who must travel long distances to a drugstore.
Maryland, New Mexico and Oregon enacted or updated laws allowing pharmacists to prescribe birth control pills, patches and other forms of contraception that do not require a doctor to administer.
The flurry of state legislative activity on women’s health issues this year is a direct result of the federal policy shifts on women’s health since President Donald Trump took office, said Danielle Wells, a spokeswoman on state policy issues for Planned Parenthood.
But she cautioned that state initiatives can only go so far to mitigate what she said would be very damaging effects on women’s health care if the federal government decides to defund Planned Parenthood.
“While it’s heartening to see state lawmakers put women’s health ahead of politics, at the end of the day, if Congress votes to prohibit individuals on Medicaid from accessing care at Planned Parenthood, no amount of state support will be able to fill that gap,” Wells said.
Without Planned Parenthood clinics, use of contraception would decline and abortion rates would likely rise, Nash said. Wider use of contraception accounted for a 14 percent drop in the U.S. abortion rate between 2011 and 2014, according to Guttmacher, and for a reduction in the rate of unplanned pregnancies as well.
But abortion opponents argue that the nation’s declining abortion rates are due to tougher state abortion laws, and they maintain that women will still be able to obtain birth control and other reproductive health services from a variety of other health care providers without funneling taxpayer dollars to Planned Parenthood.
“The issue is not contraception, the issue is why should we give the nation’s No. 1 abortion provider more than a half a billion dollars to provide a service that is better provided by other medical centers where women can receive full-service care,” said Kristi Hamrick, spokeswoman for Americans United for Life, an anti-abortion advocacy group.
Defunding Attempts
Over the last six years, a handful of Republican-led states have tried to chip away at funding for Planned Parenthood, one of the nation’s largest providers of women’s health care. The most common tactic has been to exclude the group from Medicaid’s network of providers.
Indiana was the first state that attempted to block Planned Parenthood funding, followed by Alabama, Arizona, Arkansas, Florida, Kansas, Louisiana, Mississippi, Oklahoma and Texas. In nearly every case, courts shot down their attempts to prohibit the abortion provider from participating in state Medicaid and federal grant programs.
In December, President Barack Obama signed a Health and Human Services rule clarifying that states could not block funding to health care providers for purely political reasons.
But that policy was quickly reversed when Trump took office.
Less than four months into his administration, Trump signed a law allowing states to do just what they had been trying to do for years — exclude Planned Parenthood from Medicaid and other women’s reproductive health care programs, despite a federal Medicaid statute that prohibits it.
At the same time, Republicans in Congress repeatedly have called for elimination of the roughly $300 million federal grant program known as Title X that funds Planned Parenthood and other local family planning clinics.
And in May, a leaked Health and Human Services proposal revealed that the Trump administration intends to undo a provision in the federal health law that requires nearly all employers to include coverage of all forms of contraception in their employee health plans. If the proposal takes effect, it would make it easy for employers to opt out of coverage of contraception for religious or moral reasons.
Those actions and the uncertain future of the Affordable Care Act have stripped Planned Parenthood and many other women’s health clinics of any certainty about their financial future, causing some to put off any plans for expansion.
Back to States
Despite setbacks in Iowa and other states, Planned Parenthood’s Wells says women’s health advocates have been buoyed by their successes in several GOP states — and by the overall number of women’s health initiatives this year. She attributes the unprecedented level of state activity in support of her group and its goals to a national groundswell of activism that started with the Women’s March on Washington early this year, and the momentum in state capitols that has been sustained since.
But other women’s health advocates worry that just as many states, emboldened by the Trump administration’s apparent green light on defunding women’s health, will move quickly to cripple Planned Parenthood clinics in their states.
“People should be very concerned about what states are doing around Medicaid and women’s health now that the new administration has reversed Obama-era protections,” said Mara Gandal-Powers, senior counsel with the National Women’s Law Center.
A recent poll by the Kaiser Family Foundation found that three-quarters of the American public, and a majority of Republicans, favor continuing federal funding of Planned Parenthood for non-abortion services.
At least 38 million U.S. women of reproductive age need contraceptive services because they are sexually active and do not want to become pregnant, according to Guttmacher. In 2014, more than half of them needed subsidized services because they were unable to purchase contraception on their own. Thirty-nine percent of those received care at federally funded clinics, including Planned Parenthood, or from private practice doctors serving Medicaid enrollees.
For state Medicaid programs, preventing unintended pregnancies makes financial sense. Every dollar spent on publicly funded family services yields $4 in Medicaid savings, because unintended births are avoided, according to the National Partnership for Women and Families. Total public expenditures on unintended pregnancies in the U.S. were an estimated $21 billion in 2010, nearly a third of which was state money.
The potential demise of the Affordable Care Act, with its expansion of Medicaid and required coverage of birth control for all women at no cost, represents by far the biggest potential loss to women’s health.
“Things got better under the ACA. It reset the baseline,” Gandal-Powers said. “That’s why we’re seeing such vocal and active pushback against what is happening in women’s health now.”
Kristyn Ingram and her husband Ross, with their four children. COURTESY/KRISTYN INGRAM
On the day before her abortion, Kristyn Ingram and her husband flipped through books of baby names. They chose one if it was a girl, and another for a boy.
The next morning — December 8, 2006 — Ingram, then a fourth-year medical student in San Antonio and 17 weeks pregnant, received the abortion pill cytotec to induce labor at her local hospital. She got an epidural. After 12 hours she delivered a girl, dead. They named her Annabelle Cartwright Ingram.
Ingram and her husband, Ross, wanted a baby. But a screening when she was 16 weeks pregnant found Potter syndrome, a rare condition in which fetal kidney failure prevents the lungs from developing. Knowing that the chance of survival was extremely low, the Ingrams decided to terminate the pregnancy.
“We were completely devastated,” said Ingram, who slept with Annabelle’s hospital blanket the week after. The couple wears matching rings with blue topaz — Annabelle’s birthstone. “But the idea of bringing a baby into the world to suffocate and only know pain was unacceptable.”
Ingram’s abortion was covered by her health insurance, costing her between $200 and $400 out of pocket, she told the Observer. But under a bill up for consideration in the Senate Business and Commerce Committee Saturday, Ingram said she would have been on the hook for the full cost — close to $10,000 for the second-trimester procedure and hospital stay. It’s a price tag that would have been “completely out of the realm of possibility” as a medical student paying for school, she said.
Senate Bill 8 would ban private insurance plans in Texas from covering abortion, without any exception for cases of fetal anomaly, like Ingram’s. If a person wants abortion coverage, the proposal says it “does not prevent” him or her from buying supplemental coverage outside of a qualified health plan. But the bill does not require that such plans exist. One of three anti-abortion measures on Governor Greg Abbott’s special session agenda, SB 8 does include an exception for “medical emergencies.” But under Texas law, medical emergencies are defined as a “life-threatening physical condition” that “places the woman in danger of death or a serious risk of substantial impairment of a major bodily function.” Critics say the definition is so narrow that it could force someone facing a high-risk pregnancy to pay thousands of dollars out of pocket — or put off an abortion until their life is in danger.
“This has a direct impact on access to health care in tragic circumstances … and to add insult to injury, the Texas Legislature is going to say, ‘Oh by the way, your insurance company won’t cover this safe thing that your doctor recommends,’” said Blake Rocap, legal counsel for NARAL Pro-Choice Texas. “They would have to wait until they’re basically actively miscarrying, and then it’s super dangerous — we’re talking about hospitalization; it’s much more expensive for the insurance plan, and much more dangerous for the mother to wait that long.”
Consideration of SB 8, authored by Senator Brendan Creighton, R-The Woodlands, with a House companion from Representative John Smithee, R-Amarillo, comes the day after the Senate Health and Human Services committee sent two anti-abortion bills to the full Senate for approval. On Thursday, reproductive-rights attorneys filed a lawsuit against Texas’ anti-abortion law passed during the regular session.
The measure to ban abortion coverage in private plans is a longtime favorite of anti-abortion advocates, who say they shouldn’t have to pay into health coverage that includes a procedure they vehemently oppose. A similar bill passed the Senate in the regular session, and passed out of committee in the House.“This is long overdue,” said Joe Pojman, executive director of Texas Alliance for Life.
But terminating a pregnancy is by nature unplanned. Even if supplemental abortion coverage were available, people would be unlikely to buy it, the bill’s critics say. “Most people don’t go into a pregnancy thinking something bad will happen and they’ll need to terminate — especially a planned pregnancy,” Ingram said. “I would never have bought a supplemental abortion insurance policy because I’d never have thought I’d need it.”
Kristyn Ingram and her husband Ross, with their four children. COURTESY KRISTYN INGRAM
Ingram, who turns 36 this month, has four healthy kids now, who “all know they had an older sister.” Each year on Annabelle’s birthday, the family decorates their Christmas tree with an angel ornament.
Ingram said she’s lucky to have had the resources and support she did during her abortion and that her medical background made a big difference. “I have no guilt whatsoever about my termination because I saw the ultrasound, I knew what it meant, I knew the outcome,” she said.
But had SB 8 been in place 11 years ago, she would have been in trouble.
“In medicine, we know all kinds of things can go wrong,” Ingram said. “But I had the innocence of a first pregnancy where you assume everything will go right and you’ll take home a baby at the end.”



.jpg)