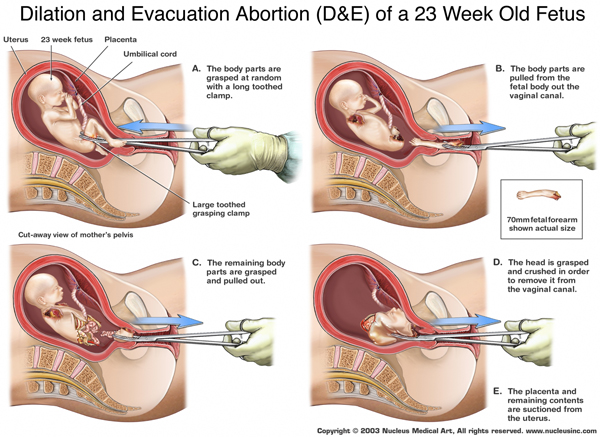
Let’s face it: most people view late term abortions as a pretty hideous thing, and that opinion is one of the few to cross the pro-choice/pro-life divide. The pro-life side is aware of this, which is why a substantial amount of propaganda focuses on the method of late term Dilation and Evacuation procedures and attempts to conflate it with earlier term abortions, to pair a false equivalence with emotional appeal. (I’ve seen the following picture—or one very much like it–shared from multiple conservative sites online, as well as handed out by abortion protesters at clinics or demonstrations.)

What has been striking to me, however, is how prevalent the ignorance of issues relevant to late term abortion tends to be on both sides of the divide. On both sides, I often encounter ignorance as to why women might choose to seek late term abortions in the first place (although this is more prevalent among pro-lifers), and about the relevant physiological details in terms of fetal development near viability.
Is there a secular argument for late term abortion bans?
Actually—surprisingly—yes. Essentially, the ethical considerations around abortion all center on the question of what defines a “person.” While it remains a hotly debated philosophical and religious question, it’s also one that we can attempt to answer scientifically. One answer is viability, and the landmark decision in Roe v. Wade adheres to this measurement. This in itself is a somewhat blurred line because each pregnancy is unique and the point at which different fetuses becomes viable is variable. Still, the court decision defined viability as between 24 and 28 weeks’ gestation. With new medical advances over time, the limit of viability (the gestational age that ensures a significant chance of survival outside the womb) has fallen to earlier in pregnancy, but a survey of just over 700 members of the American College of Obstetricians and Gynecologists (ACOG) showed that most would still not attempt to rescue fetuses younger than 24 weeks with a caesarian section if there were signs of fetal distress. Respondents who judged viability to be earlier than 24 weeks tended to have practiced for a shorter period of time and to be from southern or central states (I wonder what that could mean?).
There are other medically sound arguments that can be made, however, for abortion bans prior to viability. If we measure the beginning of meaningful life by the same benchmark we use to measure the end of meaningful life for comatose patients, a secular argument can be made that the beginning of brain function, which actually precedes viability, is more important in determining the beginning of meaningful personhood than likelihood of survival outside the mother’s body. Even here, however, the answer gets a little dicey: which benchmark is the most important to use?
From the review article “Pain and its Effects in the Human Neonate and Fetus,” we have the following description of the beginning of fetal brain function: “intermittent electroencephalograpic bursts in both cerebral hemispheres are first seen at 20 weeks gestation; they become sustained at 22 weeks and bilaterally synchronous at 26 to 27 weeks.”
Cortical functioning is crucial to higher order cognitive processes necessary to all attributes we associate with personhood (thought, memory, emotion, perception, reasoning, etc.), so using it as a measure for the beginning of meaningful personhood is sound logic, in theory. Philosopher Mary Anne Warren’s often-touted 5 criteria of personhood (consciousness, reasoning, self-motivated activity, capacity to communicate, and self-awareness), and other personhood definitions that require higher levels of cognitive or physical functioning, have troubled critics who point out that such a high bar may eliminate not only fetuses from “personhood,” but also many mentally or physically handicapped people and children up to several years of age. Lowering the bar instead to brain development necessary to support the most basic form of sentience is more inclusive: sentience is something of which all “people” are capable no matter how cognitively impaired, and in normal cases precedes other, higher forms of brain functioning. Below it, there is nothing indicative of personhood, and without it, all higher forms of awareness (such as self-awareness or the ability to reason) are impossible. This definition notably excludes those with brain death and early term fetuses.
What makes late term abortion bans a bad idea?
Despite their deep unpopularity that spans the abortion divide, and even despite a secular argument that could be used to support them, late term abortion bans are currently unfeasible, and likely a very bad idea. Why? There are several reasons:
1) Many severe fetal abnormalities can’t be caught until after the 20th week. Only about 1% of abortions are performed after the 20th week, according to the Guttmacher Institute, but many of those are due to severe developmental or genetic fetal abnormalities that are found by ultrasonography after 20 weeks. Of these, many are unsalvageable pregnancies, in which the fetus will almost inevitably die close to birth or shortly after. Forcing women to carry wanted but doomed pregnancies to term is cruel and unnecessary.
Still, in the debate for late abortion bans, there remains huge controversy about the legality of abortion for less severe defects, such as Down Syndrome. This has led, on the pro-life side, to a sometimes prevalent impression that abortions for fetal defects are never necessary, but rather an excuse for “lazy” women to get rid of children that don’t meet their ideals. North Dakota recently became the first state in the country to pass a law banning abortions because of fetal defects, and dubbed the practice a form of “discrimination.” Meanwhile, in Texas, lawmakers who recently passed a 20 week abortion ban with no exception for severe but not definitively lethal fetal defects remained deaf to testimony from women who had received late term abortions for that reason.
There are multiple problems with this particular pro-life perspective. First and foremost is the severity of the misperception of why women have abortions for non-lethal fetal defects. The blanket judgment that they are lazy or refuse to have imperfect children fails to acknowledge the very real psychological burden that mothers of impaired children bear. A study of mothers of disabled children of various types found they suffered from significantly higher psychological distress compared to other mothers, even after education, income, and race were controlled for. Many more studies of individual disorders among children (ADHD, asthma, cystic fibrosis, Duchenne muscular dystrophy—the list goes on, and yes, it includes Down Syndrome) consistently reveal poor mental health in their mothers compared to controls (depression and anxiety are most commonly studied). And while it is true that there appears to be gradation in the psychological effects on mothers concomitant with the severity of their children’s defects (for instance, one study showed Down Syndrome children’s mothers have better mental health than mothers of children with Fragile X syndrome or autism), this is no reason to discount the idea that not all women are psychologically or financially prepared to deal with raising a disabled child. (It’s also worth noting that many women can receive earlier term abortions after discovering their child has Down Syndrome, since early tests are available that can screen for it in the first trimester, so it is much less relevant to the late term abortion debate than most pro-lifers imply.)
The second problem with the pro-life view that abortions are never necessary for fetal defects is that it heavily downplays the importance of abortions of wanted pregnancies performed for almost invariably fatal defects like anencephaly, a condition (seen below) in which much or all of the brain fails to form.

Lastly, even when pro-lifers do recognize the importance of abortions for fatal disorders (instead of merely supporting perinatal hospice/palliative care instead), we run into another problem: the slippery slope. Where do fatal disorders fall that don’t cause death immediately, but invariably cause death over time? Cystic Fibrosis and Huntington Disease fall into this category, and prenatal testing options are available for both. If abortion bans are to be instated, and allow only some fetal defects to be used as an exception, who should draw the line in the sand, and where should that line be?
2) Many abortion bans make exceptions for maternal life, but not maternal health. It’s difficult to overstate the severity of this oversight. The major problem with this kind of legislation is embodied by Savita Halappanavar, who recently began a firestorm in Ireland over women’s reproductive rights. Savita sought hospital care while undergoing a miscarriage, and though her physicians were well aware her pregnancy was doomed, their hands were tied by Irish law until the fetus’s heartbeat stopped, because Savita, despite being in extreme physical pain and distress, was not deemed to be in mortal danger. Unfortunately, when the heartbeat ended and Savita’s physicians were able to intervene, it was too late: Savita died of an entirely preventable case of septicemia. If you think the case will make a difference in Ireland’s laws, I’d urge you not to hold your breath: their new law doesn’t allow exceptions for rape, incest, or even lethal fetal abnormalities, but only for the life of the mother. Unfortunately, it doesn’t actually fix the problem that led to Savita’s death: as is, the legislation still requires doctors to wait for a preventable problem to become potentially lethal before they are legally allowed to intercede.

Sadly, recent state level abortion bans in the US that make exceptions for the life but not the health of the mother suffer from the exact same problem. Addressing the Arkansas House about a recent proposed “fetal heartbeat bill,” the chairman of the Department of Gynecology and Obstetrics at the University of Arkansas for Medical Sciences (UAMS) pointed out that, under the law, doctors who perform abortions for women with congenital heart problems who have a 50% chance of surviving childbirth, or for women who suffer a rupture of the amniotic membrane surrounding the fetus (which inevitably causes miscarriage but may lead to severe infection while the fetus still lives) could be charged as felons.
3) Abortion bans are put in place without addressing the reasons women have abortions later in pregnancies besides fetal defects. A report by the Guttmacher Institute showed that black women, adolescents, women with lower levels of education, and women with insurance policies that covered abortion procedures were more likely to have second trimester abortions than other women. For the first three categories, the report may indicate significant issues in lack of access: “The overwhelming majority of second-trimester patients would have preferred to have had their abortion earlier, and our findings suggest that black women and those with less education would most benefit from increased access to early abortion services.”
Unfortunately, and ironically, anti-abortion legislation in multiple states aimed at reducing access by closing abortion clinics with unnecessary restrictions or requiring extra hurdles for women to obtain abortions (like mandatory delay, ultrasounds, and/or counseling), has a counterproductive effect. Most women affected by these laws still have abortions, but many seek them later due to their difficulty accessing services. This is further supported by a Guttmacher Institute report that studied the effects of a mandatory delay law in Mississippi on the timing of women’s abortions. It found that after the law was implemented, the rate of second-trimester abortions rose by 53% for all women who didn’t live close to an out-of-state provider! When coupled with laws aimed at eliminating early access to abortion, current late term abortion bans seem more about further preventing women from accessing abortion than a good-faith attempt at balancing women’s reproductive rights with bioethical concerns.
What does this mean for late term abortion bans?
While very strongly pro-choice, even I have serious moral qualms about the ethicality of very late term abortions in unexceptional cases, because of concerns that they may be performed after there is enough brain function to support a primitive form of sentience. Since I’m of the notion that “I think, therefore I am,” I feel there’s a serious case to be made that fetuses with intermittent or sustained cortical function (at 20 or 22 weeks’ gestation, 2-4 weeks prior to the current general bar for viability) are in fact “people.” Still, I have to say that late term abortion bans are not currently feasible, because implementing them successfully would require the type of compromise between the pro-choice and pro-life community that neither side appears at all comfortable making.
For a late term abortion ban to be at all fairly implemented, it would require the pro-choice side to give up the notion that all elective abortions should be legal up to viability. In return, the pro-life side would have to concede several things: first, that exceptions should be made for rape, incest, maternal life and health, and all fetal defects discovered by ultrasonography or prenatal testing. Second, that early term abortion access should be encouraged and expanded, making it readily available for poor and minority women. This would, of course, require overturning the many, many laws passed in recent years by the GOP at the state-level aimed at doing the precise opposite, and may even require overturning the Hyde Amendment, which bars federal funding for abortion, thus preventing poor women from receiving elective abortions except in cases of rape, incest, and their lives.
As you can see, putting in place a late term abortion ban that could actually be considered a moderate proposal and which is supported by one secular argument for personhood is a near-impossibility, as it would require actual compromise between pro-choice and pro-life legislators and the willingness to lose ground on either side. In a political climate where ‘compromise’ is a dirty word, and one side refuses to even listen to opposing viewpoints, let alone negotiate, getting to a point where both sides meet in the center will be a long, uphill battle.
References:
1) Morgan, M.A., Goldenberg, R., Schulkin, J. 2008. Obstetrician-gynecologists’ practices regarding preterm birth at the limit of viability. Journal of Maternal-Fetal and Neonatal Medicine 21(2): 115-21. http://www.ncbi.nlm.nih.gov/pubmed/18240080
2) Anand, K.J.S., Hickey, P.R. 1987. Pain and its Effects in the Human Neonate and Fetus. The New England Journal of Medicine 317(21): 1321-29.
http://www.cirp.org/library/pain/anand/
3) Mary Anne Warren’s essay “On the Moral and Legal Status of Abortion”: http://instruct.westvalley.edu/lafave/warren_article.html
4) Guttmacher Institute’s “Facts on Induced Abortion in the United States,” including rates of early vs. late term abortion: http://www.guttmacher.org/pubs/fb_induced_abortion.html
5) For more on the extreme anti-abortion laws passed by North Dakota, including one barring abortion for gender preference or genetic defects (the first of its kind in the United States): http://www.nytimes.com/2013/03/27/us/north-dakota-governor-signs-strict-abortion-limits.html?pagewanted=all&_r=1&
6) Here are several papers on the psychological effects of raising disabled children:
–Breslau, N., Staruch, K.S., Mortimer, EA Jr. 1982. Psychological distress in mothers of disabled children. American Journal of Diseases of Children 136(8): 682-6. http://www.ncbi.nlm.nih.gov/pubmed/6213143
–Yilmaz, O., Sogut, A., Gulle, S., et al. 2008. Sleep quality and depression-anxiety in mothers of chidren with two chronic respiratory diseases: asthma and cystic fibrosis. http://www.ncbi.nlm.nih.gov/pubmed/18585104
–Bourke, J., Ricciardo, B., Leonard, Helen. 2008. Maternal physical and mental health in children with Down syndrome. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2586647/
–Abi Daoud, M.S., Dooley, J.M., Gordon, K.E. 2004. Depression in parents of children with Duchenne muscular dystrophy. Pediatric Neurology 31(1): 16-19.
–Abbeduto, L., Seltzer, M.M., Shattuck, P., et al. 2004. Psychological well-being and coping in mothers of children with autism, Down syndrome, or fragile X syndrome. American Journal of Mental Retardation 109(3): 237-54. http://www.ncbi.nlm.nih.gov/pubmed/15072518
–Hobdell, E. 2004. Chronic sorrow and depression in parents of children with neural tube defects. Journal of Neuroscience Nursing 36(2). http://journals.lww.com/jnnonline/Abstract/2004/04000/Chronic_Sorrow_and_Depression_in_Parents_of.5.aspx
7) For information on prenatal testing for Huntington Disease (http://predictivetestingforhd.com/testing-for-hd/prenatal-testing/) and Down Syndrome (http://www.mayoclinic.com/health/down-syndrome/DS00182/DSECTION=tests-and-diagnosis)
8) For more information on Savita Halappanavar’s death: http://www.irishtimes.com/news/health/report-identifies-multiple-failures-in-treatment-of-savita-halappanavar-1.1427332
9) For more on the new Irish abortion bill: http://www.bbc.co.uk/news/world-europe-23507923
10) For more on Dr. Curtis Lowery’s testimony in opposition to Arkansas’ proposed fetal heartbeat bill in February: http://www.arktimes.com/ArkansasBlog/archives/2013/02/08/a-doctor-speaks-out-on-abortion-bills
11) Jones, R.K., Finer, L.B.. 2011. Who has second-trimester abortions in the United States? Contraception 85(6): 544-51. http://www.guttmacher.org/pubs/journals/j.contraception.2011.10.012.pdf
12) Joyce, T., Kaestner, R. 2000. The impact of Mississippi’s mandatory delay law on the timing of abortion. Family Planning Perspectives 32(1). http://www.guttmacher.org/pubs/journals/3200400.html
13) For more on state-level abortion restrictions so far into 2013: http://www.guttmacher.org/media/inthenews/2013/07/08/
14) Last, but certainly not least, this website is dedicated to sharing the stories of women who received late term abortions for medical reasons: http://1in10blog.wordpress.com/
Share what you read here:
 You are forever talking about what you know is right for women, what women want, and what they really need. You’ve even told clinic staff, doctors and nurses that you know they could do better in another line or work. With your particularized notion of moral righteousness, you’ve lodged complaints with police about what you know are your rights to free speech at abortion clinics. You’ve written letters to private citizens, neighbors of doctors and clinic directors, asking them to tell these professionals to find a new job, because you know better, you know what’s right. But your self-obsession as well as your presumptuous omniscience conveniently ignores the rights of others and summarily dismisses the knowledge women have of their own lives. Behaving, as you are wont to do, foolishly believing you are right when you are really wrong on so many levels, you reveal more truths about your nature than you might imagine or want. Let me spell it out for you.
You are forever talking about what you know is right for women, what women want, and what they really need. You’ve even told clinic staff, doctors and nurses that you know they could do better in another line or work. With your particularized notion of moral righteousness, you’ve lodged complaints with police about what you know are your rights to free speech at abortion clinics. You’ve written letters to private citizens, neighbors of doctors and clinic directors, asking them to tell these professionals to find a new job, because you know better, you know what’s right. But your self-obsession as well as your presumptuous omniscience conveniently ignores the rights of others and summarily dismisses the knowledge women have of their own lives. Behaving, as you are wont to do, foolishly believing you are right when you are really wrong on so many levels, you reveal more truths about your nature than you might imagine or want. Let me spell it out for you.

















 As David Gunn, Jr. wrote in a recent award-winning blog, the “Abortion Rights Freedom Ride” is on the road. They started inNew York City and San Francisco on July 23 and are headed to Fargo, North Dakota. They will then venture south through Wichita, culminating in a rally at the Jackson Women’s Health Organization in Mississippi.
As David Gunn, Jr. wrote in a recent award-winning blog, the “Abortion Rights Freedom Ride” is on the road. They started inNew York City and San Francisco on July 23 and are headed to Fargo, North Dakota. They will then venture south through Wichita, culminating in a rally at the Jackson Women’s Health Organization in Mississippi.


