Fetal parts are for sale. Yep, the terrible Planned Parenthood abortionists found and tapped into a profitable market for fetal parts, especially intact forms.
This is the basic narrative inserted into the talking points of anti-abortion politicians these days after edited videos between Planned Parenthood representatives and imposter biomedical tissue brokers surfaced. Ignored was the benefit fetal tissue provides to medical research. Disregarded was the selectivity used to decide what was fit for public consumption. Much has been made of interactions that might be suspicious to outsiders of medical and scientific research environments or appeal to the emotions of the uninformed.
Planned Parenthood can sufficiently respond to the “undercover sting videos” of its medical staff discussing fetal tissue donation. The rest of us need to respond to this attempt by anti-abortion dogmatists to impose their view of the world into public policy. The states that have initiated investigations based on the videos found Planned Parenthood in compliance with regulations. Even if one state, or several states, unsuccessfully takes action for political value or reject continued contracts with Planned Parenthood for health services, it would be a measurement of success for this false narrative. Planned Parenthood will remain open to provide important health services, but there are other issues of which we should all have concern.
Deception and Ethics
The videos were created by the Center for Medical Progress (CMP), which claims to be “…citizen journalists dedicated to monitoring and reporting on medical ethics and advances.” Their website appears to be focused only on promoting anti-abortion viewpoints, no other medical ethics issues. End-of-life treatment, organ donation processes, and equality in accessing medical care are among the top ethical issues one would expect to see mentioned.
Why the deception when it would have been perfectly acceptable for CMP to identify itself as abortion opponents with specific, legitimate ethical questions pertaining to abortion and fetal tissue?
Honesty and integrity are critical to discussions about ethical issues. Would abortion clinic representatives talk openly with abortion opponents? I and many others certainly have on many occasions in our roles as reproductive healthcare professionals. Did the CMP even attempt to arrange a discussion? If the intent of the “undercover” effort was to learn about the involvement of some Planned Parenthood affiliates with fetal tissue procurement, it was not necessary for CMP to engage people by misrepresenting themselves as biomedical professionals. Why just Planned Parenthood and no other providers of elective, therapeutic, and emergency abortions? Hospitals and other medical facilities play a significant role in tissue procurement, which can seem quite unsavory to outsiders.
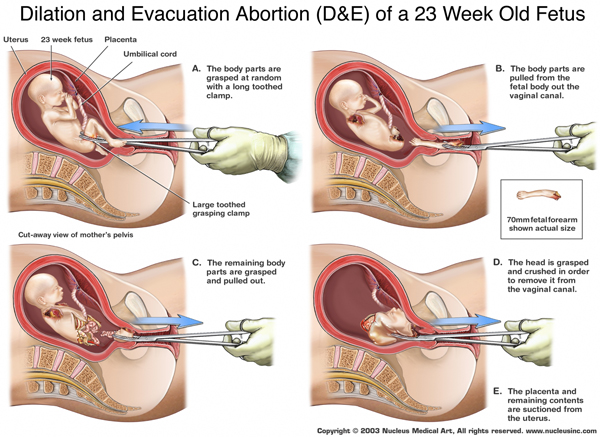
 Apparently deception and fabrication are a preferred method of operation within anti-abortion activism. Deception and fabrication are the hallmarks of Crisis Pregnancy Centers, also known as fake abortion clinics because of the their strategy to appear as if they are abortion clinics and use misinformation to dissuade women from abortion once they arrive for their “abortion appointment.” Anti-abortion literature distributed to Congress, the media, and the public also contains incorrect, distorted, and often manufactured information. This is how the public at times believes that most abortions are late term. Or have murky ideas about parental consent for abortion in which it is compared to unrelated issues that are often guided by business policies, not laws.
Apparently deception and fabrication are a preferred method of operation within anti-abortion activism. Deception and fabrication are the hallmarks of Crisis Pregnancy Centers, also known as fake abortion clinics because of the their strategy to appear as if they are abortion clinics and use misinformation to dissuade women from abortion once they arrive for their “abortion appointment.” Anti-abortion literature distributed to Congress, the media, and the public also contains incorrect, distorted, and often manufactured information. This is how the public at times believes that most abortions are late term. Or have murky ideas about parental consent for abortion in which it is compared to unrelated issues that are often guided by business policies, not laws.
It is no surprise that deceptive tactics were used to generate the storyline about fetal tissue procurement. It is nonetheless striking that there is not outrage about the deception, especially when ethics is the alleged target. Clearly, acquiring and providing information about fetal tissue procurement would not generate outrage if done without the theatrics of imposter biomedical professionals and video editing skills. Do we really want topics of importance to be introduced to public discourse in this manner? Of course not. The media would serve the public well to fully investigate the “investigators” and bring political balance to that part of the story. The notion that an organization like CMP, with a Postal Annex rented address no record of prior work as a nonprofit in the medical ethics arena, and leadership comprised of people connected to anti-abortion groups like Operation Rescue, can have traction in promoting political ideology as if it was credible news or journalism is frightening. The media failed by not scrutinizing the source before doing the reporting, especially since another group, Life Dynamics, attempted to do the same in the late nineties.
For the record, pro-choice people resorted to deception to “out” the Crisis Pregnancy Center’s fake abortion clinic charades. Why? Because CPCs claimed that they informed women that they did not perform abortions, provided factual information, and other practices did not square with what women had shared with actual medical professionals. A hidden camera sent in by the media with a young woman proved that the experiences of other women were accurately presented.
Using the Mistruths as Truths to Further the Mistruths
Talk radio stars Laura Ingraham, Sean Hannity, and Rush Limbaugh all regularly speak of the CMP as if it is a credible nonprofit out there doing good work. Politicians, including U.S. Speaker of the House John Boehner and those running for president, refer to the videos time and again as if they were part of a documentary. Absolutely nothing revealed in the videos is evidence of anything sinister. At worst, the videos illustrate the seeming insensitivities that can develop when people work in medical settings. wd
Right wing websites are having a great time exaggerating the video content and piling on more false or misleading information. Red State claims that Planned Parenthood was “…caught…appearing to haggle over the sale of aborted baby parts.” Haggling? Not hardly. The videos revealed explanations, in clinical and business tones, about how tissues and parts are procured. Bear in mind that CMP presented themselves as biomedical professionals interested in obtaining fetal tissue. Would it have somehow been acceptable for responses to exclude information about quality of parts and associated costs?
Comments made by elected officials can be perceived as the truth. Thus, when Senate newcomer Joni Ernst (R-Iowa) states, “Planned Parenthood is harvesting the body parts of unborn babies,” to explain her sponsorship of a bill to defund Planned Parenthood, perceptions are broadly formed and shared throughout every possible medium. The tone of Ernst’s statement can conjure so many images that only perpetuate incorrect information. When Breitbart News quotes a Ted Cruz comment that the videos show Planned Parenthood representatives “confessing to multiple felonies,” it misleads, misinforms, and further polarizes people on the basis of ideology as opposed to facts. Shame on all who have made, and are continuing to make, comments implying that the videos exposed evidence of crime. Shame on all who are giving the CMP credibility, so much credibility that there are threats to shut down the government if Planned Parenthood is not defunded.
Fetal Tissue Research is Ethical and Beneficial
There has always been a market for anatomical and biological goods, including human fetal tissue and parts. Specific companies respond to the demand for human and animal parts. College psychology departments buy brains to teach students. Medical and scientific researchers need specimens in order to learn more about genetics or real and prospective treatment options for a range of diseases, for example. Fetal tissue/parts obtained from miscarriages and abortions have been used for decades and have led to a number of medical breakthroughs, including rubella and polio vaccines. Kimberly Leonard wrote an excellent article in the August 4, 2015 online issue of US News about the contributions of fetal tissue research. Many of us are grateful for those contributions. In the August 12, 2015 New England Journal of Medicine, lawyer R. Alta Charo stated, “A closer look at the ethics of fetal tissue research…reveals a duty to use this precious resource in the hope of finding new preventive and therapeutic interventions for devastating diseases. Virtually every person in the [United States} has benefited from research using fetal tissue.” Quite simply, it would be unethical for medical researchers to suddenly discontinue use of fetal tissue due to politically extreme ideology.
 Fetal parts are not allowed to be sold – they can only be donated with consent from pregnant women after they are removed. If profit for fetal parts is the actual concern of CMP, their time would be better spent honestly working with regulatory agencies to determine with certainty if any inappropriate financial transactions between abortion providers and biomedical tissue businesses exist. It is certain that people of all political views on the issue would abhor such a practice.
Fetal parts are not allowed to be sold – they can only be donated with consent from pregnant women after they are removed. If profit for fetal parts is the actual concern of CMP, their time would be better spent honestly working with regulatory agencies to determine with certainty if any inappropriate financial transactions between abortion providers and biomedical tissue businesses exist. It is certain that people of all political views on the issue would abhor such a practice.
As the dribble of videos continues, no evidence of illegal activities will be presented. Instead, ideology will be promoted with the intent to cause some to rethink their views about abortion and try to stop an organization that serves the healthcare needs of so many low-income women. The effort will fail, but in the meantime, we will all have to witness the nonsense and speak up about reality when we can.

 National Right to Life, Family Research Council, and other anti-abortion organizations have been enthusiastically spreading the word about a study published in the New England Medical Journal showing that a fetus can be viable if born at 22 weeks gestation with advanced medical intervention. A
National Right to Life, Family Research Council, and other anti-abortion organizations have been enthusiastically spreading the word about a study published in the New England Medical Journal showing that a fetus can be viable if born at 22 weeks gestation with advanced medical intervention. A