Most American women between 15 and 49 years of age use birth control, according to a new U.S. government report.
Between 2017 and 2019, 65% of those women used some form of contraception, according to the U.S. Centers for Disease Control and Prevention.
“This report provides this unique snapshot of all women of reproductive age at a point in time,” said lead researcher Kimberly Daniels. She’s a demographic statistician at the CDC’s National Center for Health Statistics (NCHS) in Hyattsville, Md.
The most common types of birth control were female sterilization (18%), oral contraceptive pills (14%), long-acting reversible contraception, or LARCs (10%), and male condoms (8%).
LARCs—which include intrauterine devices and under-the-skin implants—were most popular among women in their 20s and 30s. Among 20- to 29-year-olds, 14% used LARCs, as did 13% of women in their 30s. LARCS were the method of choice for 6% of 15- to 19-year-olds and 7% of women in their 40s, the findings showed.
Hispanic and Black women were more likely to rely on condoms (11%), compared with white women (7%), the researchers found.
And women with more education preferred contraceptive pills over sterilization, the study found.
“The less commonly used methods in terms of percentages would be natural family planning and diaphragms,” Daniels said.
The last time Daniels looked at contraceptive use was 2018, and the most common methods are still the same. Understanding contraceptive use across populations sheds light on fertility patterns, including birth rates and unintended pregnancies, she said.
The report was published Oct. 20 in the CDC’s NCHS Data Brief.
Dr. Jill Rabin, co-chief of ambulatory care and obstetrics and gynecology at Northwell Health in New Hyde Park, N.Y., reviewed the findings.
“Contraception is an individual choice which is dynamic and changes with people’s lives and the desire for fertility or needing to protect against an unintended pregnancy,” Rabin said.
Half of all pregnancies in the United States are unintended—but that doesn’t mean “unwanted,” Rabin said.
“A significant portion of people who are not using contraception are either seeking fertility or not actively seeking to become pregnant, but if they did become pregnant, they would be happy,” she said.
Many people who don’t use birth control are LGBTQ or don’t have heterosexual sex, she added.
One of the main barriers for women who want contraception is cost, Rabin said. Whether a woman has health insurance or not can determine what type of birth control is available to her.
Condoms are cheap and readily available, but birth control pills and LARCs require a prescription and are costly, which limits their availability to many poor and uninsured women, Rabin said. “And abortion is not a method of birth control,” she added.
While effective in preventing pregnancy, Rabin cautioned that contraceptives do not protect against sexually transmitted infections (STIs).
“The STI rate is way too high. Even condoms are not 100% effective against sexually transmitted infections,” she said.
Justice Amy Coney Barrett has officially been confirmed to the Supreme Court of the United States, filling the seat once held by Justice Ruth Bader Ginsburg. Barrett was confirmed on Monday with a 52-48 Senate vote (the first time in 151 years a justice was confirmed with zero support from the minority party), eight days out from the November election.
While Barrett, who has now cemented the Supreme Court’s 6-3 conservative majority, is poised to rule on a number of issues that could affect our lives in the immediate—the Affordable Care Act, absentee ballot deadlines in essential swing states—when the nation first heard of Ginsburg’s passing, the future of Roe v. Wade was top of mind. President Trump previously promised to nominate judges with the intention of overturning Roe, the 1973 ruling that confirmed the constitutional right to abortion.
So now that Barrett is on the court, what does that mean for the future of abortion rights? Here, what you need to know.
Where does Amy Coney Barrett stand on abortion?
Barrett, a conservative Catholic, is known to be personally anti-abortion. She has said she believes “life begins at conception,” and in 2006, she signed her name to an ad that opposed “abortion on demand.” She is also an originalist, meaning she “interprets the Constitution according to the understanding of those who drafted and ratified it,” according to the New York Times.
In a 2013 law review article, she wrote: “I tend to agree with those who say that a justice’s duty is to the Constitution and that it is thus more legitimate for her to enforce her best understanding of the Constitution rather than a precedent she thinks clearly in conflict with it.” In 2016, NPR reports she said, “I don’t think the core case, Roe’s core holding that women have a right to an abortion, I don’t think that would change. But I think the question of whether people can get very late-term abortions, you know, how many restrictions can be put on clinics, I think that will change.”
Though Barrett, who joined the U.S. Court of Appeals for the 7th Circuit in 2017, does not have an extensive judicial record, according to Vox, she has twice voted in favor of abortion restrictions. (Read more about the specific cases, here.)
Throughout her confirmation hearing for the Supreme Court, Barrett did not directly say how she might rule on Roe or abortion rights. However, as stated above, she’s made clear that she’s open to reversing precedent if she believes that decision is in conflict with the Constitution.
Nancy Northup, the president and CEO of the Center for Reproductive Rights, a legal advocacy organization, told ELLE.com: “The confirmation hearing made clear that Judge Barrett has the most extreme record and opposition to reproductive rights of any SCOTUS nominee in three decades.” She continued, “You can see it in her approach to Constitutional interpretation, you see it in her opinions on the Seventh Circuit, and she had vitriolic public advocacy defending the right to life from fertilization. That is a straight-on legal perspective that is not consistent with the Supreme Court’s jurisprudence recognizing that the right to access abortion and contraception is protected in the 14th amendment. I think states are going to open the floodgates for those that want to restrict access to abortion. They’re going to see this opportunity with her on the court.”
What could happen to Roe v. Wade with Barrett on the court?
It’s essential to note that abortion rights can be stripped away without Roe being overturned—and it’s already happening across the country. There are bans on when you can have an abortion, the type of abortion you can have, and barriers to access, like long waiting periods.ADVERTISEMENT – CONTINUE READING BELOW
A number of states also have Targeted Regulation of Abortion Providers (TRAP) laws that advocates say chip away at abortion access and ultimately intend to shut down abortion providers. Planned Parenthood describes TRAP laws as “costly, severe, and medically unnecessary requirements imposed on abortion providers and women’s health centers,” such as creating building requirements for clinics or requiring abortion providers to have admitting privileges at nearby hospitals. For example, in 2016, the Supreme Court struck down a Texas law in the case Whole Woman’s Health vs Hellerstedtthat would have required providers to have admitting privileges; even though the law was ultimately deemed unconstitutional, before the Supreme Court even ruled, it caused half of the state’s abortion-providing clinics to close. (Also, since these laws are introduced at the state level, it is essential to vote down-ballot in the upcoming election if you are concerned about electing pro-choice state leaders.)
When it comes to what Barrett could soon rule on, according to CBS News, there are 17 abortion-related cases that are one step from the Supreme Court. Two others have already reached the court, though it’s yet to be announced whether they will hear arguments for either case. One of those cases is a 15-week abortion ban in Mississippi that CBS reports challenges the core holding of Roe, which legalized abortion until fetal viability, usually around 24 weeks of pregnancy. (The Supreme Court, including Justice Barrett, will be considering that petition this Friday.) Northup said the 15-week abortion ban “is a straight-on challenge to Roe v. Wade” and that “the court cannot uphold it without reversing Roe v. Wade.” Beyond those 17, there are dozens of others cases currently making their way through the judicial system, including six-week abortion bans, which also present a direct challenge to Roe. (For more information, on what could happen in your particular state if Roe were to be weakened or overturned, check out the Center for Reproductive Rights’ interactive map, “What If Roe Fell?”)
When it comes to reproductive rights, we must also consider the issue of healthcare, especially as the Supreme Court is set to hear a challenge to the Affordable Care Act this November. “The Affordable Care Act has probably been the most significant advancement of women’s reproductive healthcare since Roe,” Northup said. As she explained, more people are covered under the ACA due to the Medicaid expansion and the affordability of insurance, meaning more are getting maternal healthcare. Insurance companies can no longer exclude people who, for example, have had C-sections from receiving pregnancy care, and the law’s no copay contraception guarantee allows many to get their choice of contraceptive without cost.
How to help:
According to Northup, this is now the “most conservative court on abortion rights, probably since Roe.” So what can you do? “The vast majority of the nation wants abortion to be safe and legal, and it really matters to make that support visible,” she said. “Everything from talking to family, friends, and co-workers, to making that support visible on social media, to making that support public with protests and being out there on the streets—all of those are very, very important. It matters the context in which this will be decided.”
You can also donate to an abortion fund, which assists patients in securing and paying for abortion care. The Cut has created an extensive guide to abortion funds in states considered “hostile,” meaning lawmakers will try to prohibit abortion if Roe falls, and states considered “not protected,” meaning places where abortion will not have legal protection if Roe falls. You can also find abortion funds across the country through the National Network of Abortion Funds.
Vote down-ballot in the upcoming election, and urge your representatives to support laws like the Women’s Health Protection Act, which would protect people’s access to abortion “by establishing federal statutory rights for providers to provide and patients to receive abortion care free from medically unnecessary restrictions and bans,” according to the Guttmacher Institute.
The inflammatory phrase seeks to politicize a situation that can cause unimaginable suffering for pregnant people.
Opponents of abortion have long tried to stigmatize the medical procedure, but in the past few years, they’ve targeted abortions performed in the second and third trimester. President Donald Trump and Vice President Mike Pence have repeatedly claimed that Democratic lawmakers support “late-term abortions” done “up to the moment of birth.”
Doctors, meanwhile, have repeatedly explained that they do not perform abortions while people are in labor, or in the days before their due date, but the talking point persists. “My patients didn’t ask to be spoken about this way, they didn’t ask for their health care to be politicized, and they’re the ones that are suffering the most from all of this,” Jen Villavicencio, MD, MPP, an ob-gyn and abortion provider in Michigan and the Darney-Landy Fellow at the American College of the American College of Obstetricians and Gynecologists, tells Health.
“Inflammatory language like ‘late-term abortion’ is used to deflect the conversation away from the safe, legal provision of compassionate medical care to patients,” Dr. Villavicencio says. Here, ob-gyns and abortion providers cut through the political talking points and focus on the facts regarding abortions later in pregnancy. This is what you need to know.
What do politicians mean when they say ‘late-term abortion’?
In short, it’s a sensationalized phrase that doesn’t reflect science or medicine. While people may have heard physicians use “late term” in a medical setting, it refers to women in the 41st week of their pregnancy, that is, women who are still pregnant after their due date, and no abortions occur during this time period, Dr. Villavicencio says. Physicians instead say “abortions later in pregnancy” or “later abortions,” or simply refer to the trimester when the procedure happens.
What is a later abortion, and how often does it happen?
It depends on who you ask, but generally later abortions are those that happen after a specific point in pregnancy (for example, beyond 20 weeks or in the third trimester) or after a fetus is viable, which is thought to be at about 24 weeks though that’s not a hard and fast rule. There is no magic switch that flips in the same week of every pregnancy after which that fetus is viable; viability is determined by a physician on an individual basis.
Abortions in the second trimester are most often done via a procedure known as dilation and evacuation, or D&E, where the cervix is dilated either with medication or seaweed sticks known as laminaria that swell and open the cervix, and then the pregnancy is removed through the cervix using instruments. Abortions in the third trimester, which are a very small number of procedures, involve inducing labor, Daniel Grossman, MD, and ob-gyn and abortion provider and a professor of obstetrics at the University of California San Francisco and director of Advancing New Standards in Reproductive Health (ANSIRH), tells Health.
These later abortions are rare: According to the Centers for Disease Control and Prevention, in 2016, just 1.2% of abortions were performed at 21 weeks of pregnancy or later. Another 7.7% were done from 14 to 20 weeks, while the vast majority, 91%, were performed at or before 13 weeks. Put another way, this means 98.7% of all abortions happen before 21 weeks. Dr. Grossman says there isn’t great data on the breakdown of procedures after 21 weeks but, he says, “it’s clearly much less than 1% past 24 weeks.”
Given that these later procedures are so uncommon, Dr. Villavicencio says: “The political focus on abortion later in pregnancy does not reflect the medical reality and disproportionately impacts those who find themselves in need of critical healthcare.”
Why do people get later abortions?
There are several reasons why people have later abortions, and they generally fall into two categories. “It’s either due to some new information that has come about during their pregnancy or a result of barriers that exist to getting abortion,” Dr. Villavicencio says.
The “new information” category includes learning something about the health of the fetus or the pregnant person, but it also encompasses people not realizing they’re pregnant until later on. This can happen because they’re using birth control, they have irregular periods, or they’re young and not aware of pregnancy symptoms, Dr. Grossman says. Dr. Villavicencio says she’s had abortion patients who are grandmothers and didn’t think they could get pregnant. Late recognition of pregnancy is “not unusual, and certainly not a fault of someone for not knowing. Unless you’re taking a pregnancy test every single month, which no one does, it’s very easy to miss a pregnancy,” she says.
Fetal health problems could include a malformation of the fetus or genetic abnormality that means the fetus won’t survive. But these problems often aren’t diagnosed until later in the second trimester or into the third because the screening tests and scans don’t pick these problems up until that late, Dr. Grossman says. The special ultrasound that’s colloquially known as “an anatomy scan“—where the fetus is large enough that doctors can see the heart, brain and spine—isn’t usually done until 18 or 20 weeks, but can be as late as 23 weeks, based on the availability, where a person lives, or even what’s going on in their life, Dr. Villavicencio says. Then if the scan does pick up something concerning, people need time to get a specialist appointment for a second opinion.
Similarly, people can develop dangerous health complications in pregnancy that may not emerge until the later second trimester or early third trimester. Two examples are pre-eclampsia, or high blood pressure later in pregnancy that can become life-threatening, and placenta previa, when the placenta is covering the opening of the uterus and can cause severe bleeding during pregnancy. The treatment for these conditions is delivery and C-section, respectively, Dr. Grossman says, but if the patient is still in their second trimester and the fetus isn’t viable, abortion is sometimes the best option for their health.
Barriers to accessing care can also push people who want abortions to get them later in pregnancy. These obstacles include living far away from an abortion clinic thanks to anti-abortion clinic shutdown laws, facing a medically unnecessary state-mandated waiting period of 24 to 72 hours that requires multiple trips to a clinic, and the costs associated with that travel such as gas, hotel stays, childcare (60% of people seeing abortions already have kids), and unpaid time off from work. Plus if you’re having an abortion procedure rather than getting the abortion pill to take at home, you might need someone to travel with you, Dr. Villavicencio says.
Another is the cost of the procedure itself—an average of just over $500 at 10 weeks in 2014—which may not be covered by health insurance, especially for people living on low incomes who have Medicaid. Thanks to the 1976 Hyde Amendment, the federally funded Medicaid program can only cover abortions in the cases of rape, incest, or threat to the mother’s life. States can use their own funding to cover the procedure, but only 16 do so while 34 states and Washington, DC, stick to the federal standard, according to the Kaiser Family Foundation. Because of structural racism, Black and Latinx women are more likely to have Medicaid insurance and are thereby less likely to have the procedure covered.
The price of the procedure is, of course, added to any travel costs mentioned above. “That is a real, real barrier for many patients,” Dr. Grossman says. “[The Hyde Amendment is] a common reason why people end up presenting for care in the second trimester because it took time for them to get the funding together to be able to pay for the abortion.” And the later an abortion is, the more expensiveit is, so the problem snowballs.
By contrast, in a 2012 study in the American Journal of Public Health, Dr. Grossman found that in the two years after Iowa made early medication abortions easier to access through a telemedicine program, that people were almost 50% more likely to have a first-trimester abortion while second-trimester abortions declined, even after controlling for other factors.
“I think there’s a lot of evidence showing that these restrictions can push people later in pregnancy and increase the likelihood that they’ll get a second-trimester abortion, and conversely, that efforts to expand access to early abortion can help to reduce second-trimester abortion,” Dr. Grossman says.
Which states restrict later abortions?
Forty-three states ban abortion after a specific gestational age, with 17 banning it after 20 weeks, while seven states do not have gestational limits, according to the Guttmacher Institute.
Under the Supreme Court rulings Roe v Wade and Planned Parenthood v Casey, states can only ban abortion after the fetus has reached viability, meaning it could survive outside the womb, as long as there are exceptions to save the life and health of the mother. That framework means state bans after viability don’t have to permit exceptions for people who faced barriers to getting care or those whose fetuses have severe anomalies.
Of the 17 states with 20-week bans in effect, 13 lack exceptions for lethal fetal anomalies, meaning people who want abortions in those cases would have to travel out of state. States that have passed bans before viability have typically done so in an effort to provoke a Supreme Court challenge, per Guttmacher. Gestational age bans also ignore the medical reality that some pregnancies will never be viable.
What do politicians mean when they talk about babies “born alive” in abortions?
President Trump has also repeatedly claimed that doctors are delivering healthy babies and then “executing” them, which does not happen.
There are rare cases where the fetus has been diagnosed with a severe condition that is clearly incompatible with life. After counseling with their medical team and specialists, some patients choose to induce labor, knowing that the fetus will not survive after delivery, and offer comfort care. This is called perinatal palliative care and it’s an accepted medical practice, Dr. Grossman says. Sometimes people choose to induce labor rather than having a D&E procedure because they want to hold their baby or because the labor process will be cathartic for those who were preparing to deliver, Dr. Villavicencio says.
Dr. Villavicencio says these are “heart-wrenching, tragic” situations where the decisions made are no different than other end-of-life care—it’s just that this is at the other end of the spectrum of life. Families are deciding whether they want to take futile steps like intubation and CPR or let their loved one pass away peacefully. But crucially, “it is not medical dying and it’s not physician-assisted suicide and it is not hastening the death of anyone in any way,” she says. “This is purely a way to offer as much comfort as possible while the inevitable occurs.”
These are not abortions of healthy pregnancies. “This is not ‘hey by the way, I forgot I want an abortion.’ They’ve had conferences with the neonatal intensivists, with the obstetricians, with the pediatricians, with the palliative care team to discuss how and when this palliative birth is going to occur,” Dr. Villavicencio says. “If [politicians] were being honest about what they were talking about, they wouldn’t be talking about ‘moment of birth,’ because that’s not when the abortion decision is being made.”
With abortion foe Amy Coney Barrett newly minted as a Supreme Court justice, we’re bracing for impact.
Amy Coney Barrett was sworn-in as a Supreme Court justice on Monday. She’ll begin to consider cases by the end of the week. Tasos Katopodis/Getty Images
I have a question.
Is Mississippi OK? Not the people in Mississippi. There are lots of good people in Mississippi. But I mean public officials in Mississippi. Like the governor. And the attorney general. And basically any attorney representing Mississippi in court.
Because not only have they ignored my plea to stop filing Supreme Court petitions, they actually upped the ante by filing a supplemental brief containing “legal” arguments (please read those quotation marks as sarcastically as possible), which supposedly explain why the state’s unconstitutional 15-week gestational ban is actually constitutional. In making its “legal” arguments, Mississippi blabbers on for seven blissfully short pages, managing to cram in a lot of bullshit about cases that have nothing to do with Mississippi’s case.
And frankly, it’s starting to make me lose my mind a bit.
Mississippi’s case, Jackson Women’s Health Organization v. Dobbs, is about a 15-week gestational ban, yet another flavor of pre-viability abortion ban anti-choice numpties like to cook up. Under current abortion law, pre-viability abortion bans are unconstitutional. The Supreme Court has ruled over and over again that states cannot outright ban abortion before viability.
Everyone agrees—Mississippi’s lawyers included—that no fetus is viable at 15 weeks. Mississippi’s law is therefore unconstitutional. Period. That’s why the district court struck it down. And that’s why even the extremely conservative Fifth Circuit Court of Appeals struck it down.
But Mississippi doesn’t have to convince the district court or the Fifth Circuit that its “legal” arguments are sound. Mississippi has to convince the Supreme Court, where a new justice was installed on the bench just yesterday to destroy access to health care, including abortion care. If Mississippi’s lawyers give newly minted Justice Amy Coney Barrett an abortion turd, she’ll find a way to polish it into an abortion stone.
So, what did attorneys for Mississippi do last week as Barrett’s nomination was barreling through the Senate? They filed a nonsense supplemental brief discussing how the federal courts have been ruling in recent cases involving TRAP laws (targeted regulations of abortion providers).
TRAP laws are laws that regulate only abortion providers. Mississippi’s abortion ban is not a TRAP law. An abortion ban is a law that … well … bans abortion—like Mississippi’s 15-week ban.
In cases involving TRAP laws, courts have to do an undue burden analysis. Planned Parenthood v. Casey, a case almost as foundational to abortion rights as Roe v. Wade, requires it.
And right now there’s a live fight about what kind of undue burden analysis courts need to do, thanks to Chief Justice John Roberts leaving a ticking time bomb in his concurring opinion in June Medical Services v. Russo this summer. Roberts may have helped Louisiana clinics stay open in the short term, but his ruling will likely end up wiping out clinic access across the country. It’s already being used to wipe out access in Kentucky.
But none of this should have anything to do with Mississippi’s case. Mississippi’s case is about a pre-viability ban. The TRAP law cases are about abortion regulations. There’s no need for an undue burden analysis when it comes to pre-viability bans because they are unconstitutional.
But no. Mississippi Attorney General Lynn Fitch has been desperately trying to get someone to buy her argument that the abortion ban isn’t really a ban. It’s a regulation. And if it’s not a regulation, it’s at most, a partial ban. And besides, Casey doesn’t ban all pre-viability abortion bans!
But that’s exactly what Casey does.All of this nonsense is a transparent effort to prime the pump so that when Justice Barrett is seated, Mississippi and every other state controlled by anti-choice forces can float any bullshit argument before the Supreme Court.
The Supreme Court in Casey said, “viability marks the earliest point at which a State’s interest in fetal life is constitutionally adequate to justify a legislative ban on nontherapeutic abortions.”
A state can start banning abortion after fetal viability. Not before.
That’s it. End of discussion. Everyone go home.
But Mississippi doesn’t want to go home. Mississippi wants the Court to analyze its pre-viability ban as if it were a TRAP law. If Mississippi can convince a court to apply the undue burden test to all abortion restrictions—including already unconstitutional pre-viability abortion bans—then Mississippi’s 15-week ban might stand a chance.
After all, you can’t even get an abortion in Mississippi after 16 weeks. Anti-choice legislators in Mississippi have made sure of that. So when you think about it, a 15-week ban is only a burden—if you can even call it that—for a week. And how many pregnant people will that even affect? It’s too few to even bother counting.
That’s Mississippi’s argument. And it might seem like a reasonable one if you ignore what the court in Casey said: “Our adoption of the undue burden analysis does not disturb the central holding of Roe v. Wade, and we reaffirm that holding.”
Got it? The Casey Court reaffirmed the holding of Roe. And what is that holding, pray tell?
“Regardless of whether exceptions are made for particular circumstances, a State may not prohibit any woman from making the ultimate decision to terminate her pregnancy before viability. “
One more time!
“A State may not prohibit any woman from making the ultimate decision to terminate her pregnancy before viability. “
Nuh-uh, says Mississippi in court documents filed with the Supreme Court. “Regulations designed to foster the health of a woman seeking an abortion are valid if they do not constitute an undue burden.”
But Mississippi’s law isn’t a regulation. It’s a fucking ban.
Well fine, then, Mississippi flounces. “It’s a ban. But it doesn’t matter anyway because viability is the wrong standard. It’s outdated. Please, oh please, Justice Barrett, won’t you hear our cries and upend the foundation of abortion rights jurisprudence?” (Attorneys for Mississippi didn’t actually say this, but they may as well have since this will be one of the very first cases that Justice Barrett will consider.)
Is it obvious that Mississippi is getting on my goddamn nerves? Because Mississippi is getting on my goddamn nerves.
All of this nonsense is a transparent effort to prime the pump so that when Justice Barrett is seated, Mississippi and every other state controlled by anti-choice forces can float any bullshit argument before the Supreme Court and be relatively confident that the conservative supermajority, all of whom hate abortion, will buy it.
All these states need to do is give the conservative justices on the Supreme Court enough cover so that when they reverse either Roe and Casey—or interpret one or both cases in a way that further guts access to abortion care—states like Mississippi can implement laws that for more than 40 years have been unconstitutional.
And with the Supreme Court scheduled to discuss on Friday whether to take this case, Mississippi may get its wish.
Senate Republicans are poised to confirm President Trump’s Supreme Court nominee Judge Amy Coney Barrett on Monday, a major victory for the President and his party just days before November 3, that promises to push the high court in a more conservative direction for generations to come.The stakes in the Supreme Court battle are immense and come at a pivotal time in American politics in the run up to an election where control of Congress and the White House are on the line.
Trump’s appointment of a new Supreme Court justice will mark the third of his tenure in office, giving Republicans a historic opportunity to deliver on the key conservative priority and campaign promise of transforming the federal courts through lifetime appointments. Trump is expected to swear-in Barrett at the White House in an outdoor ceremony at 9 p.m., Monday, after her expected confirmation, a source familiar with the invitation tells CNN.
Barrett, who is 48 years old, is likely to serve on the court for decades and will give conservatives a 6-3 majority on the Supreme Court, a shift in its makeup that will have dramatic implications for a range of issues that could come before it, including the future of the Affordable Care Act and any potential disputes regarding the 2020 election.
Senate Republicans, who hold a majority in the upper chamber, have pushed ahead with one of the quickest nomination proceedings in modern times following the death of the late Justice and liberal icon Ruth Bader Ginsburg last month.They have the votes to confirm Barrett over the objections of Democrats who have argued that the process has been a rushed and cynical power grab that threatens to undermine Ginsburg’s legacy.
“The Senate is doing the right thing. We’re moving this nomination forward and, colleagues, by tomorrow night we will have a new member of the United States Supreme Court,” Senate Majority Leader Mitch McConnell said on Sunday after the Senate advanced the nomination in a key procedural vote to break a Democratic filibuster.The confirmation battle has played out in a bitterly-divided Senate, but the outcome has not been in question for much of the fight. With few exceptions, Senate Republicans quickly lined up in support of Barrett after her nomination by President Trump. All Democrats are expected to vote against the nomination.Two Republican senators crossed party lines to vote with Democrats in opposition to Sunday’s procedural vote — Susan Collins of Maine and Lisa Murkowski of Alaska.
Collins, who is facing a competitive re-election fight, is expected to vote against the nomination over concerns that it’s too close to Election Day to consider a nominee. Murkowski has already announced, however, that she will ultimately vote to confirm Barrett in the final vote, but said that she would vote against the procedural vote after having previously voiced opposition to taking up a nominee to fill the open seat so close to the election.Senate Republicans have largely rallied around the nomination, however, praising Barrett as exceedingly qualified to serve on the Supreme Court. Republicans, who have a 53-seat majority, only need 51 votes to confirm a new justice.
Senate Democrats, in contrast, have decried the nomination and the confirmation process.Democrats have warned that Barrett’s confirmation will put health care protections and the Affordable Care Act in jeopardy. They have argued that the confirmation process has been rushed and accused Republicans of hypocrisy in moving ahead with the nomination after blocking consideration of former President Obama’s Supreme Court nominee Merrick Garland in 2016.
“The Republican Party is willing to ignore the pandemic to rush this Supreme Court nomination forward,” Senate Democratic leader Chuck Schumer said in a floor speech on Sunday.Democrats, who are in the minority, have been limited in their ability to oppose the nomination, but have protested the process in a variety of ways.
When the Senate Judiciary Committee voted to advance the nomination, Democratic senators on the panel boycotted the vote, filling their seats instead with pictures of people who rely upon the Affordable Care Act in an effort to draw attention to an upcoming case on the health care law’s constitutionality and their arguments that Barrett’s confirmation would put the law at risk.During confirmation hearings, Democrats sought to elicit answers from Barrett on a number of controversial topics the Supreme Court could take up. Barrett repeatedly declined, however, to specify how she might rule on a range of topics, from the Affordable Care Act to Roe v. Wade and the high court’s ruling legalizing same-sex marriage.
Barrett explained during the hearings that she shared a philosophy with the late conservative Justice Antonin Scalia, whom she clerked for, but argued she would not be an identical justice if she is confirmed.
“If I’m confirmed, you would not be getting Justice Scalia. You would be getting Justice Barrett,” she said. “And that’s so because originalists don’t always agree.”
Women in Texas can continue to access the most common procedure used to end a pregnancy in the second trimester, after a federal appeals court Tuesday struck down a state law that would have curtailed its use.
A nurse practitioner consults with a patient at a Planned Parenthood clinic in Austin. Credit: Tamir Kalifa for The Texas Tribune
Women in Texas can continue to access themost common procedure used to end a pregnancy in the second trimester, after a federal appeals court Tuesday struck down a state law that would have curtailed its use.
The law would have required doctors to stop the fetus’s heart before performing a dilation and evacuation abortion — in which doctors use surgical instruments to remove pieces of fetal tissue — except in the case of a medical emergency. Those who violated the law could have faced prison time.
The measure — which never went into effect — has been tied up in litigation since the Texas Legislature passed it in 2017. It was struck down by a district judge in Austin, who said it substantially burdened a woman’s right to an abortion, and was appealed before the politically conservative 5th U.S. Circuit Court of Appeals in New Orleans. The proceedings were stalled pending a Supreme Court case decided this summer.
Judge James Dennis, writing for the majority, said the law “forces abortion providers to act contrary to their medical judgment and the best interest of their patient” by first stopping the fetus’s heart with procedures that are “unfeasible,” “dangerous” and provide “no benefit to the woman.”
The requirement could increase the duration of an otherwise one-day dilation and evacuation procedure, potentially burdening low-income women who “must wait until the second trimester to seek an abortion because of the time needed to obtain funds to pay for the procedure,” he wrote.
The law’s “burdens substantially outweigh its benefits,” he wrote. The decision was 2-1, with two Democrat-appointed judges in the majority and Republican-appointed Judge Don Willett dissenting.
The state’s lawyers have likened the method of a dilation and evacuation to “dismemberment,” and Attorney General Ken Paxton has called it “barbaric.”
Abortion providers who brought the lawsuit say dilation and evacuation is the safest way to end a second-trimester pregnancy and that an effective ban on it would subject women to medically unnecessary and untested procedures. The requirement to stop a fetus’s heart could lead providers to “essentially experiment” on patients, one doctor said in a trial about the law in 2017.
Molly Duane, an attorney with the nonprofit Center for Reproductive Rights, said the alternative to a dilation and evacuation procedure is medical induction — “essentially giving birth.”
“Labor induction, just practically speaking, isn’t available in Texas, let alone logistically speaking. Asking a patient to exchange a simple outpatient, 10-minute procedure for hours if not days inpatient in the hospital — again in the middle of a pandemic — is unrealistic,” she said in an Aug. 12 interview.
The American College of Obstetricians and Gynecologists has said the procedure is “evidence-based and medically preferred” because it results in the fewest complications for women in the second trimester.
Tuesday’s decision comes after the 8th U.S. Circuit Court of Appeals lifted a block on four Arkansas abortion restrictions in August, citing Chief Justice John Roberts’ opinion in the recent Supreme Court case June Medical Services v. Russo. While Roberts’ crucial vote in that case awarded a victory to advocates of abortion access then, he issued a narrow opinion that said lawmakers have wide discretion “in areas where there is medical and scientific uncertainty” and that weighing the “costs and benefits of an abortion regulation” was not necessarily a job for the courts.
Lawyers representing Texas argued this presents a different standard than was applied by the district court that struck down the dilation and evacuation restriction in 2017. In that ruling, the burdens of the law were weighed in relation to its benefits — a balancing test rejected by the June Medical decision, the state’s lawyers wrote.
“The Chief Justice demonstrated that is it not enough to show merely that a law imposes some ‘burden’ on abortion access, or that a regulation makes abortion more difficult or expensive. … Rather, ‘the only question for a court is whether a law has the ‘effect of placing a substantial obstacle in the path of a woman seeking an abortion of a non viable fetus,’” the state’s lawyers wrote, citing Roberts’ opinion.
The court disagreed, with Dennis writing that the judges agreed the “balancing test still governs.”
Katie realized she was pregnant during the first week of April 2020. She decided pretty quickly that she wanted to terminate the pregnancy. She already had two kids, and she’d just been diagnosed with high blood pressure. The condition was still uncontrolled, which made her pregnancy high-risk. But it was just weeks into the COVID-19 pandemic in the U.S. She was in full lockdown, and she wasn’t sure if she could get an abortion.”I was Googling abortions,” she tells Refinery29. “My biggest thing was not wanting to actually go to a place.” Besides being afraid of catching the virus, the nearest clinic to Katie was six hours away from her home in New Mexico, and she wasn’t sure how she’d find the time to get there.
Her internet research led her to the website for the TelAbortion Study. If she participated, she’d be able to receive the pills necessary for a medication abortion — a procedure that uses medication to end a pregnancy — through the mail, and have consultations with her doctors via the phone. Besides an ultrasound, which she could obtain at a nearby facility, she’d never have to leave her house.
Less than three weeks later, in late April, she began her abortion by taking mifepristone, a drug that blocks progesterone, a hormone needed for pregnancy to continue. The following day, a Friday, she took misoprostol, which induced uterine contractions to help her body expel the tissue. And that was it. “I laid in bed and [the medication] kind of just took its course. I cramped a little bit,” she says. She had taken that Friday off work, and her children (ages 3 and 7) were at their father’s house for the weekend. “I liked the fact that it was in the comfort of my own home,” she says. “I was able to do it on my own time.”
Over 1 In 3 Abortions Use This Pill. Why Is It So Heavily Restricted?
In 2017, medication abortions accounted for 39% of all abortions in the U.S., according to the Guttmacher Institute. When used during the early stages of gestation (up until around 11 weeks), the drugs are safe and effective. A patient is given an ultrasound or blood test to confirm they’re eligible before being prescribed the drugs — mifepristone and misoprostol — along with a pain medication like ibuprofen and an anti-nausea medication, explains Kristina Tocce, MD, MPH, vice president and medical director of the Planned Parenthood of the Rocky Mountains, a TelAbortion provider. The provider may offer birth control counseling or prescriptions, as well. One to two weeks after the abortion, the patient has a follow-up appointment.
Unfortunately, like all abortion care in the U.S., medication abortion is subject to restrictions that limit people’s ability to access the treatment.In 2011, the FDA imposed a Risk Evaluation and Mitigation Strategy on Mifeprex, the brand name for mifepristone. (The other abortion drug, misoprostol, is prescription-only, but not regulated by a REMS.) As a result, the medication must be dispensed by a certified provider in a clinic, hospital, or medical office. That means patients generally can’t be prescribed via telemedicine, or receive the drug via the mail — or even at a retail pharmacy. What’s more, in order to carry the drugs, physicians are required to be included on a list of certified abortion providers. Many are reluctant to do so, fearing backlash, according to an article published in the New England Journal of Medicine. All this can make the medication difficult to get. “It is needlessly stressful to have to establish care with a new medical provider for such a private, yet simple medical service,” says Melissa Grant, COO of Carafem, a network of healthcare providers working with TelAbortion. The REMS seems restrictive for a drug that’s largely seen as safe. “To date, 19 deaths have been reported to the FDA among the more than 3 million women in the United States who have used Mifeprex,” write the authors of the NEJM article. “In contrast, the background risk of pregnancy-related death among pregnant women in the United States who do not have abortions and instead proceed to live birth is… 14 times higher.” A study of 8,765 telemedicine and 10,405 in-person medical abortions found “a very low prevalence of clinically significant adverse events among patients undergoing medical abortion,” reports the journal Obstetrics & Gynecology.
The TelAbortion Study can get around the REMS because it’s a clinical study, and therefore granted an exemption, says Inga Platais, a senior program associate at Gynuity Health Projects, the non-profit organization sponsoring the TelAbortion Study. Since 2016, the project has been allowed by the FDA to provide abortion medication via mail to patients in Colorado, Georgia, Hawaii, Illinois, Iowa, Maine, Maryland, Minnesota, Montana, New Mexico, New York, Oregon, Washington, and the District of Columbia. “We are currently exploring expansion into additional states,” Platais says. They’ve been able to work with residents who live in other states but are able to travel to a participating state on a case-by-case basis.
Dr. Tocce recalls treating a patient from Texas, where abortions were deemed “non-essential” during the pandemic by Governor Greg Abbott. “They traveled 10 hours by car through difficult weather conditions. They had a disabled family member and their caregiver in the car with them, and they stayed in a hotel in New Mexico [to receive treatment].” Dr. Tocce says that while it was frustrating that their option required the patient to travel, she was glad that they were able to travel the smallest distance possible. “The patient was so appreciative,” she says. “We were so thankful that we could help this person.”
How Activists Are Using COVID-19 To Push For Change
Reproductive rights advocates have long pushed for lower restrictions around abortion medication, given its safety and efficacy. Now, pressure created by the COVID-19 pandemic has opened the door to legislative change.
In late May, the American Civil Liberties Union filed a lawsuit on behalf of a coalition of medical experts led by the American College of Obstetricians and Gynecologists meant to challenge the FDA’s restrictions on mifepristone, which can also be used to manage miscarriages. The ACLU claimed that not allowing patients to be prescribed the medicine via telehealth and to fill the prescription by mail during the pandemic subjects them to unnecessary risk. (The organization filed a similar suit against the FDA — minus the COVID-19 concerns — in 2017. It is still pending.)
The most recent lawsuit stated that: “Plaintiffs have submitted evidence that 75% of women obtaining abortion care are poor or low-income and 60% are people of color, and that these populations face a significantly higher health risk from COVID-19 and in turn face particularly significant transportation, childcare, and economic challenges during the pandemic that make accessing in-person care particularly difficult and dangerous.”Federal U.S. District Judge Theodore Chuang ruled in favor of the ACLU, finding that the in-person requirements for those seeking medication abortions impose a “substantial obstacle,” and are likely unconstitutional under the circumstances of the pandemic. Until the public health emergency is over (it was renewed for 90 days on October 2), the FDA will not enforce its REMS regarding the abortion pill. Chuang says, however, that states could still oversee abortion medication “above and beyond” the FDA’s rules, The Hill reports.
While ACOG called the ruling “a victory” in a statement, Marjorie Dannenfelser, the president of an anti-abortion organization, Susan B. Anthony List, expressed disappointment in her own statement, calling the original FDA regulations “reasonable and necessary to protect women from serious and potentially life-threatening complications of abortion drugs, including intense pain, heavy bleeding, infection, and even death.
“Grant tells Refinery29 that she’s seen a “significant” uptick in clients since the pandemic hit, and has added two additional locations from Carafem into the study. “We’ve seen an increase in the number of clients asking for this, from maybe a couple a week to three times that right away. And now it’s gone up even more,” she says.Grant says that the pandemic simply magnified an existing issue around access. “People who are pregnant that are low income, who live in a place that might be cut off from medical providers, who are of color, or who don’t have reliable transportation, find it much more difficult to access an abortion,” she says. Already, she says that 30% of the network’s Georgia- and Illinois-based patients have to drive over 100 miles to reach the states’ health centers, because they don’t have any other choice.
“Now [during the pandemic], people have lost their jobs, people have lost their access to reliable childcare,” Grant notes. “Oftentimes kids are not in school or maybe their daycare situation has changed. So they’re trying to juggle that.” Telemedicine abortion care could be a life-changer.A
While research studies like the TelAbortion project and emergency rulings like the FDA’s response to the ACLU lawsuit earlier this year are a positive sign, Grant hopes that access isn’t rolled back again once the pandemic passes. “This has potentially allowed greater access to more people,” Grant explains of the ruling. “We’re hopeful that that will be an option that people can continue to access.”
Opponents Don’t Care About Science. They Just Want To Take Away Access
There is, of course, opposition to allowing medication abortion to take place via telemedicine — or really, to take place at all. “Pregnancy is not a life-threatening illness, and the abortion pill does not cure or prevent any disease. Make no mistake, Mifeprex [the brand name of mifepristone] is a dangerous pill. That’s why 20 of my Republican colleagues and I are urging @US_FDA to classify it as such,” Senator Ted Cruz tweeted in September. Attached to the Tweet is a letter from Cruz and 20 Republican senators to FDA commissioner Stephen Hahn, MD, asking the FDA to remove the drug from the U.S. market entirely. They say that Mifeprex is a “significant threat of danger.”The data suggests that Cruz and his like-minded colleagues are wrong. “It is incredibly frustrating to try to be regulated by individuals that don’t have a medical background,” Dr. Tocce says. “It’s exceptionally frustrating because the safety of medication abortion has been shown so thoroughly in so many studies, and this is literally a barrier for barrier’s sake.”
“We’ve shown so far that it’s equally effective to receive your medication at home through the mail,” Grant adds. In 2011, a systematic review conducted by the World Health Organization found that, “There is no evidence that home-based medical abortion is less effective, safe or acceptable than clinic-based medical abortion.”The TelAbortion Study has been collecting data to further demonstrate that medication abortion is safe, and can be safely carried out via telemedicine, since 2016. “Four years,” Platais says. “How much longer are we going to have to do this to show that it’s safe?
“Dr. Tocce says that speaking with the TelAbortion Study patient has been a heartwarming experience. “I’ve seen people sitting on their couch, hugging their cat and being with their children and not having to worry about, ‘How am I going to coordinate and pay for childcare while I have this visit?'” she says. “I’ve seen people in their cars during a break from work. It just really works for the patients. This is truly the definition of meeting patients where they are.
“Katie would recommend TelAbortion to anyone considering a medical abortion. She says her providers were warm and kind, which she appreciated. And while she was a little worried about using the medications correctly, ultimately she found the process simple, and she says the abortion wasn’t painful. “It’s nice to be in the comfort of your own home, and I guess… Not that people judge you over it, but…” Katie pauses, searching for the right word. “It felt safer. That’s the word I was looking for: safer.”
Republicans on the Senate Judiciary Committee voted unanimously on Thursday to advance the nomination of Judge Amy Coney Barrett to the Supreme Court over a boycott from the committee’s Democrats.
The vote paves the way for the full Senate to confirm Barrett to the high court on Monday, ahead of the Nov. 3 election between President Donald Trump and former Vice President Joe Biden.
Trump has repeatedly pressed for Barrett to be placed on the high court in time to resolve any election-related litigation, a request that Democrats see as a plain call for the court’s conservative majority to declare him the winner.
Republicans on the Senate Judiciary Committee voted unanimously on Thursday to advance the nomination of Judge Amy Coney Barrett to the Supreme Court over a boycott from the committee’s Democrats.
The vote paves the way for the full Senate to confirm Barrett to the high court on Monday, ahead of the Nov. 3 election between President Donald Trump and former Vice President Joe Biden.
Trump has repeatedly pressed for Barrett to be placed on the high court in time to resolve any election-related litigation, a request that Democrats see as a plain call for the court’s conservative majority to declare him the winner if the outcome is contested.
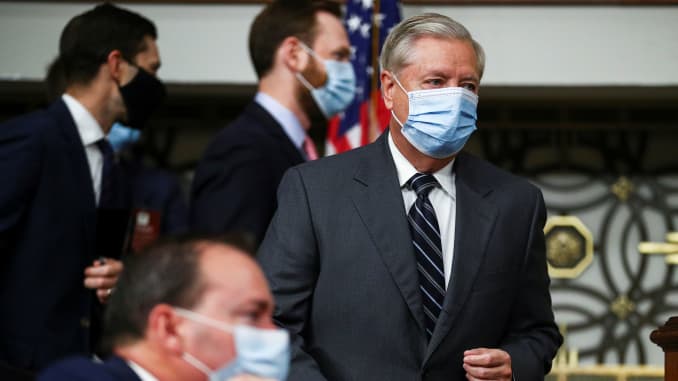
The swift action by Senate Majority Leader Mitch McConnell, R-Ky., and Judiciary Committee Chairman Lindsey Graham, R, S-C., to meet Trump’s deadline will make Barrett the first justice in history to be confirmed so close to Election Day.
Senate Judiciary Committee Chairman Lindsey Graham (R-SC) arrives next to U.S. Senator Mike Lee (R-UT) for a Senate Judiciary Committee meeting on the nomination of Judge Amy Coney Barrett to be an associate justice of the U.S. Supreme Court on Capitol Hill in Washington, U.S., October 22, 2020.Hannah Mackay | Reuters
Barrett, who was a professor at Notre Dame Law School until Trump nominated her to serve on the 7th U.S. Circuit Court of Appeals approximately three years ago, will be the sixth Republican-appointee on the nine-judge Supreme Court, and Trump’s third nominee.
Trump nominated her to the high court last month after the death of Justice Ruth Bader Ginsburg, a liberal icon who served on the bench for 27 years. Ginsburg expressed a dying wish not to be replaced until after the election.
As Ginsburg’s replacement, Barrett is expected to shift the court’s center of gravity decisively to the right, potentially imperiling the Democratic agenda items on health care, abortion access and the Second Amendment.
In focus is a Nov. 10 case the court will hear over the constitutionality of Obamacare, also known as the Affordable Care Act.
While the Democrats did not appear at Thursday’s committee hearing, they left supersized posters of individuals who rely on the law in their seats. Republicans denounced the gesture as theatrics.
Democratic Senators on the Senate Judiciary Committee boycott the committee vote on Amy Coney Barrett to serve as an associate justice on the Supreme Court of the United States during a Senate Judiciary Committee Executive Business meeting in Washington, D.C., U.S., October 22, 2020.Caroline Brehman | CQ Roll Call | Reuters
Barrett declined to provide specifics about her views on Obamacare during two days of questioning before the committee last week, but reaffirmed her originalist method of interpretation and her affinity for the late Justice Antonin Scalia, the conservative hero for whom she clerked early in her career.
Despite her previous writings that were critical of Obamacare, the conservative said she would approach the Nov. 10 case with an open mind if confirmed. She noted that the upcoming case raises questions about a legal doctrine upon which she had not previously expressed an opinion.
Some progressives were outraged by Democrats’ handling of Barrett’s confirmation hearings, arguing they lent legitimacy to a process at odds with McConnell’s 2016 refusal to even hold hearings for President Barack Obama’s nominee Judge Merrick Garland.
Organizations with power on the left, including Justice Democrats and Demand Justice, have since called for Sen. Dianne Feinstein, D-Calif., the committee’s top Democrat, to step down.
Democrats on Wednesday announced that they would boycott Thursday’s hearing.
“We will not grant this process any further legitimacy by participating in a committee markup of this nomination just twelve days before the culmination of an election that is already underway,” Senate Minority Leader Chuck Schumer, D-N.Y., said in a statement that was joined by the committee’s Democrats.
At the start of the hearing, Graham addressed Democrats’ boycott, saying “we are not going to allow them to take over the committee.”
Poland had just over 1,000 legal terminations in 2019 and rights groups say tens of thousands of women go abroad for abortions every year
Poland’s top court has ruled that abortions in cases of foetal defects are unconstitutional.
Poland’s abortion laws were already among the strictest in Europe but the Constitutional Tribunal’s ruling will mean an almost total ban.
Once the decision comes into effect, terminations will only be allowed in cases of rape or incest, or if the mother’s health is at risk.
Rights groups had urged the government not to increase restrictions.
The Council of Europe’s commissioner for human rights said the day marked a “sad day for women’s rights”.
“Removing the basis for almost all legal abortions in Poland amounts to a ban and violates human rights,” Dunja Mijatovic wrote on Twitter.
A legal challenge against the 1993 law permitting abortion in cases of severe foetal disabilities – which accounts for 98% of terminations carried out in Poland – was launched by MPs from the ruling nationalist Law and Justice party last year.
A majority of the court’s judges were nominated by the same party.
What court’s decision means for Poland
Almost all legal abortions in Poland are performed on the grounds of foetal defects, so this ruling, which is final and binding, effectively bans pregnancy terminations.
Poland is one of Europe’s most strongly Catholic countries, but there was no public clamour for this. For years opinion polls said a clear majority of Poles opposed a more restrictive law.
Bishops and lay Catholic groups pressured the governing Law and Justice party to impose a stricter law. The party supports traditional Catholic values but changing it was problematic. There was opposition both in parliament and on the streets. In 2016 an estimated 100,000 people, mostly women, protested to block an attempt to tighten the law.
image captionActivists held socially distanced protests against the proposals earlier this year
Late last year a group of governing party and far-right MPs decided to ask the court to decide the issue. This was convenient because a majority of the court’s judges were nominated by Law and Justice. It would also avoid a stormy and emotional parliamentary debate and accompanying anger on the streets in those pre-Covid days.
Now, with public gatherings limited to a maximum of 10 people in most major cities, opponents of this change will have to find other ways to show their anger.
There were just over 1,000 legal pregnancy terminations in Poland last year.
Compare that with this statistic: women’s rights groups estimate between 80,000 and 120,000 Polish women a year seek an abortion abroad. Even women who qualify for a legal procedure often face challenges to having one: such is the stigma surrounding the issue.
Malgorzata Szulecka, a lawyer for the Helsinki Foundation for Human Rights, told the BBC: “This is a totally unjustified decision that will lead to inhuman treatment of women.”
Ahead of the ruling, Polish sexual and reproductive health and rights activist Antonina Lewandowska told the BBC that the defence of the 1993 law was based on UN rules outlawing torture.
“It’s inhuman, it’s despicable honestly to make anyone carry a pregnancy to term, especially if the foetus is malformed, and 98% of legal abortions carried out in Poland are due to foetal malformations,” she said.
International human rights groups opposed the government’s stance, with Amnesty International, the Center for Reproductive Rights and Human Rights Watch saying they would send independent monitors to the court.
“The Constitutional Tribunal’s upcoming proceedings take place in the context of repeated government attacks on women’s rights and efforts to roll back reproductive rights, as well as legal and policy changes that have undermined the independence of the judiciary and rule of law in Poland,” they said in a joint statement.
Angel Kai’s* heart sank when she found out she was pregnant again. The 20-year-old had delivered her second child only three months prior. She was on unpaid maternity leave from her job in Amarillo, TX, and she’d just received a $130 electricity bill in the mail that she didn’t know if she’d be able to pay. “Everything that was happening financially was just bad,” she remembers. “I couldn’t have another kid. I knew getting an abortion would be the best thing, because I couldn’t walk up the street to get a soda if I wanted one at the time. We were that tight on money.”
It turned out, though, that Angel couldn’t even afford the abortion she knew she wanted. Her health plan was offered under state-funded Medicaid, which, in Texas, only covers abortion in cases of life endangerment, rape, and incest. So, Angel Googled “abortion financial help.” She came across a few different nonprofits called abortion funds, which provide financial assistance to people who can’t afford to go through the process themselves. One, Fund Texas Choice, said they would help Angel. They ended up footing the bill for the gas it would take to drive to the clinic, an overnight hotel stay, and her food for the trip. They also connected her with another fund that helped pay for the pill she was prescribed.The morning of her abortion, Angel dropped her baby off with a relative at 6 a.m. Then she put in a shift at the lawn company where she worked, her first since going on maternity leave. After clocking out, she started the four-and-a-half-hour drive to Albuquerque, NM. (The closest in-state clinic to her was in Dallas, an additional hour away.) Her then-partner was supposed to join her, but they got in a fight on the way, and she had to turn around and drop him off. She barely made it to the clinic on time, but she got there. And it changed her life for the better, she says.
Before finding Fund Texas Choice, Angel had tried to get an ultrasound at a “crisis pregnancy center,” which is actually a coded name for an anti-abortion clinic. “They told me abortion is murder, and that I would go to hell if I had one,” Angel remembers now, a year later. “But I knew the abortion was the best thing for me to do.” Angel’s story could have looked very different. If she hadn’t learned about the fund, she may have not been able to get the abortion pill. Alternatively, if she lived in a different state, she may have been able to use her health insurance to pay for the abortion, at a clinic much closer to her house.
In reality, the state of abortion access in America is woefully unequal. And soon, considering the tenuous status of Roe v. Wade, abortions may become even less attainable.
If Abortion Is Legal, Why Is It So Hard To Access?
In September 2020, Supreme Court Justice Ruth Bader Ginsburg died at age 87. This opened up a spot on the Supreme Court, and President Donald Trump quickly nominated conservative judge Amy Coney Barrett to fill Ginsberg’s seat. Many fear that Barrett’s appointment could lead to Roe v. Wade, the landmark 1973 Supreme Court decision that legalized abortion in the U.S., being overturned. While this possibility has led some to envision a future reminiscent of an episode of The Handmaid’s Tale, the reality is that some people who already find it easy to get an abortion — those with wealth, power, and connections — may not notice such a big change in a post-Roe world. The ones who will be hit the hardest are those who already struggle to get abortion care. Namely, low-income people in states with already-restrictive abortion legislation.
“Over the last few decades, Roe has been an unfulfilled promise for many,” says Jessica Arons, senior advocacy and policy counsel for reproductive freedom at the American Civil Liberties Union. States in the South and the Midwest tend to have the most restrictions around reproductive rights. The Bible Belt is known for legislation that typically makes abortions more expensive and time-consuming, and therefore less accessible. For instance, 34 states and Washington, D.C. only provide healthcare funding for abortions in the most extreme circumstances, such as rape or life endangerment. This is in accordance with the Hyde Amendment, which was passed just three years after Roe v. Wade legalized abortion. This is, in part, why Angel couldn’t use her Medicaid insurance to pay for her abortion.Nearly half of abortion recipients live below the federal poverty line, according to the Guttmacher Institute’s 2014 Abortion Patient Survey, so the Hyde Amendment is particularly damaging. Those who are denied abortions are more likely to experience years-long economic hardship, according to a 2017 analysis from The American Journal of Public Health. The 16 states that let Medicaid be used for most “medically necessary” abortions, (a broad definition that includes physical, emotional, familial, and psychological factors) are largely liberal states.
Another way state governments restrict access is through overly punitive regulations that are often called TRAP laws, short for Targeted Regulation of Abortion Providers. They’re medically unnecessary, and make it harder and sometimes impossible for clinicians to offer abortion care, according to The Planned Parenthood Action Fund. That can limit the number of clinics in some areas. Five states have only one remaining abortion clinic: North Dakota, South Dakota, Missouri, Mississippi, and West Virginia. People living in these states might have to travel up to 200 miles to reach a clinic, and could have to wait a few weeks for an available appointment.
In 2019, the average woman of childbearing age lived 25 miles away from the nearest abortion clinic, according to data from the journal Contraception. But that number doesn’t tell the whole story. Large cities with clinics have high populations concentrated in one area. Although the mean travel distance for a person in New York was five miles, it was 136 for a woman in South Dakota.What’s more, some states have mandatory 24-hour waiting periods or require counseling before going through the process. That means patients may have to make two individual trips to the clinic, or get a hotel and stay overnight. The trips, plus the cost of the medical regimen or procedure — which can be $1,000 or more — can be untenable without financial aid. “Across the country, we’ve already seen a systematic chipping away at the right to access abortion, even without overturning Roe,” explains Rachel Sussman, The Planned Parenthood Action Fund’s vice president of state policy and advocacy. “Since the 2010 elections, we’ve seen 480 state-level abortion restrictions passed.” The legislation disproportionately affects Black women and people of color, says Marcela Howell, president and CEO of In Our Own Voice, the National Black Women’s Reproductive Justice Agenda. Some of the states with the most restrictions have higher POC populations. In Mississippi, for instance, which upholds the Hyde Amendment and requires patients to undergo counseling before having an abortion, 38% of the population is Black, according to the U.S. Census Bureau. “Roe is the floor, not the ceiling,” Howell says. “What we’re concerned about is: How do we grant access to that right for everyone?”
And the future of abortion rights is looking bleaker and bleaker by the year, many abortion rights advocates say. In 2019, 58 new restrictions were enacted, including 25 abortion bans in 12 states, according to the Guttmacher Institute. They seek to place limitations on how, when, or why an abortion is performed. Some of the bans offer “exceptions” for pregnancies that occur due to rape or incest, but only if the patient has filed an official police report. Alabama has proposed a ban that would prohibit all abortions — period. All this is to say, access to abortion is already compromised, and that’s with the Roe v. Wade decision intact. “Yes, we all have a constitutional right to abortion, but the access has never been equally shared,” Howell says. “Women who are poor, those who have the kind of jobs that don’t have flexible hours to go to a clinic in states where they need to wait 24 to 48 hours between the initial appointment and procedure — they don’t have access.”
What Will Happen If Roe v. Wade Is Overturned?
At the first presidential debate in September Trump said, “there is nothing happening” with Roe v. Wade, and that he didn’t “know [Barrett’s] view on” the landmark ruling. But, during her confirmation hearings last week, Barrett noted “Roe is not a super-precedent because calls for its overruling have never ceased.” The prevailing belief is that the ruling is in grave danger of being overturned, Arons says. Perhaps unsurprisingly, at least some anti-abortion advocates are happy with Barrett’s appointment. “Americans United for Life was the first pro-life group to urge the president to select Judge Barrett,” Catherine Glenn Foster, president & CEO of the anti-abortion organization, told Refinery29 in a statement. She noted it’s likely the Supreme Court will have the opportunity to rule on questions of abortion rights. “We are confident that if confirmed to the Supreme Court, Judge Barrett would prove herself a trusted caretaker of the constitutional protections extended to every human person in America,” Glenn Foster said.
The Supreme Court may get its chance to reconsider Roe v. Wade within the next year, according to multiple experts Refinery29 spoke to. “Right now, there are 17 abortion-related cases that are one step away from the Supreme Court,” Sussman says. “There are several cases that could give the court the opportunity to completely gut Roe or perhaps overturn it.” That’s more likely to happen if Barrett is confirmed. Barrett has not returned a message Refinery29 left with the United States Court of Appeals for the Seventh Circuit requesting comment.If Roe v. Wade was overturned, abortion wouldn’t become illegal across the nation overnight. However, “trigger laws” that are on the books now would go into effect and ban the procedure almost immediately. And, more broadly, access would be even more dependent on state legislation than it is now, says Noel León, interim director of state abortion access at the National Women’s Law Center. Some states may pass bills or change their constitutions to protect access. Others, such as New York (where abortion was legal even before Roe was decided), have already passed laws to protect access in the event the landmark case is overturned. Meanwhile, other states could further curtail access or ban abortions completely. Without Roe, abortion would likely become illegal in 22 states, according to a recent analysis from Middlebury College. In that case, for 41% of women of childbearing age, the nearest abortion clinic would close. They’d then have to travel and average distance of 280 miles to the nearest one — compared to 36 miles, the current average for counties where a Roe reversal is likely to occur, explains Caitlin Knowles Myers, a professor of economics at Middlebury College.
And even if Roe is not overturned in one fell swoop, states could continue passing legislation that chips away at access bit by bit, and the Supreme Court could uphold those state laws, explains Laurence H. Tribe, university professor of constitutional law emeritus at Harvard. If Roe is dismantled, Sussman says that 25 million women of reproductive age live in a state where abortion would be banned.
This is perhaps the most likely scenario: That a more conservative Supreme Court will first “hollow out” Roe until there’s almost nothing left. That could look like banning common procedures for abortion, such as Dilation and Evacuation, or even forbidding abortions after brain waves are detected, Tribe says.
Right now, with the 17 abortion-related cases held up in federal appeals courts, the Supreme Court has what Tribe describes as a “menu” of cases, and they’ll get to pick and choose which to take. “They’re going to be looking for cases that will give them the maximum opportunity to do the most damage to Roe v. Wade,” Tribe says. “You’ve heard of death by a thousand cuts? That’s what may happen to Roe, after about a dozen decisions over the next three to four years.” If that occurs, or in the case of overturning Roe entirely, Congress could try to enact a national law protecting the right to abortion. “But the Supreme Court with three Trump-appointed Justices, plus Justices [Samuel] Alito and [Clarence] Thomas might hold that it’s beyond Congress’s power under the interstate commerce clause to pass such a law,” Tribe adds. Then, determining access would be in the hands of the states.
But it won’t necessarily stay with them. If Roe is eventually overturned, a more liberal state, say California, could write in their constitution that it’s still legal to have an abortion in the first two trimesters. But eventually, anti-abortion advocates could take a case to the Supreme Court saying that’s depriving the fetus of its “right to life.” “That kind of argument, which would have gone nowhere five or 10 years ago, might well have five justices behind it if Barrett is confirmed,” Tribe says. Congress could also pass a federal abortion ban that the president signs. The worst possible outcome is a sweeping constitutional amendment banning abortion federally, according to Talcott Camp, the chief legal and strategy officer at the National Abortion Federation — though she doesn’t see it happening in the near future. However, it’s been part of the Republican platform for years. “We are confronting a world in which women can be controlled by people in power,” Tribe says.
But no matter which scenario actually becomes reality, abortion access will continue to affect people unequally. “You’ve got to hold two things at once,” Camp says. “It would be a terrible, tragic loss if Roe was overturned, and that would have a huge impact on low-income, Black, brown, and rural women. But it is also true that those folks are already suffering from lack of abortion access today. And that they would suffer disproportionately were the courts to hollow out Roe so much that states could effectively ban abortion.”
Organizations that help fund abortions, like the one Angel used, are already struggling to meet the needs of their communities. “Here’s the reality a lot of people aren’t talking about,” says Laurie Bertram Roberts, executive director of both the Mississippi Freedom Fund and the Yellowhammer Fund in Alabama. Roberts, who uses she/her and they/them pronouns, has been helping low income folks pay for abortions in the South since 2013. “People are saying, ‘Well, we’ll just get money together and drive all these people to states where abortion is legal like we did before Roe,'” Roberts says. “As I always say when something is ridiculous, ‘That’s cute.’ Capacity-wise, clinics could not afford to take all of those patients. Even if we all had private jets to fly people out of state, it still would not solve the problem.” As Roberts says, “You’re gonna see folks who, with Roe, could swing it not be able to swing it any more.” The same person who could drive from Texas to New Mexico for an abortion may not be able to make it all the way to Chicago. And definitely not to Europe.This may prompt more women to try terminating their pregnancies at home, says Jen Villavicencio, MD, MPP, a physician providing abortions in Michigan and a fellow of the American College of Obstetricians and Gynecologists.
“There’s evidence to suggest that self-managed abortion — whether done with guidance from others, or done by a woman herself — can be done safely,” Dr. Villavicencio says. “I worry about the stigma associated with this… We’re in a scary place where people will potentially not be willing to seek care if they have one of the few rare complications because they’re afraid of the consequences. There are laws that exist right now that criminalize this, and people have been put in jail for it, taken away from their families.” Even though abortion is legal, there have been numerous attempts to charge and convict women for self-inducing abortion. Arons says that Black and brown women are at heightened risk for being targeted by overzealous prosecutors misusing statutes to criminalize behavior during pregnancy. States with abortion bans held up in courts right now, such as Alabama, claim they’d only prosecute doctors, not pregnant people seeking abortions. “But how would you enforce that?” asks Mary Ziegler, a law professor at Florida State University and author ofAbortion and the Law in America: A Legal History of the Abortion Debate. “People are going to fly out of state or order abortion pills online. If you’re Alabama, you’re faced with this choice: Do you not enforce your law, or do you punish your patients? That’s going to be a zero-sum decision.”
All this may seem dismal, but not all is lost, advocates say. “There are certainly states looking to protect abortion rights right now,” says Elizabeth Nash, the interim associate director of states issues at The Guttmacher Institute. “Virginia just rolled back restrictions such as counseling and waiting period requirements this year, and expanded access to abortion. In that state, 10 years ago you wouldn’t have thought that was possible, but it shows that progress can be made.”
But those advancements won’t happen if people don’t make their voices heard and vote, says Rachel Fey, the senior director of public policy at Power to Decide. She urges people to learn where their national and local candidates stand on the right to choose before casting a ballot. She notes that folks can call their Congresspeople to voice support for bills that aim to protect reproductive rights. Two are currently in the House of Representatives: the Women’s Health Protection Act, which would stop restrictions that block access to abortion care; and The EACH Woman Act, which would eliminate restrictions on abortion coverage in public and private insurance plans. Tribe adds that it’s not too late to continue to push your senators to hold off on the confirmation of Barrett before the vote on Oct. 22. “If there was a massive uprising and people realized what was at stake for them, and marched on Washington on reproductive rights, who knows?” Tribe says. “She will likely be confirmed very narrowly, and, at this point, only political pressure will matter. There’s no procedure or silver bullet available to stop this nomination. Rising up is the only way.”
What To Do If You Need An Abortion (Or Know Someone Who Does)
These days, most people who need an abortion start in the same place as Angel: Google. But it can be hard to decipher your state’s laws, and sometimes doing so takes time that you may not have. Luckily, there are organizations that make it easier.
To find the abortion clinic nearest to you, visit the National Abortion Federation’s website or call them at 1-877-257-0012, Roberts suggests. They have a list of certified clinics on their website, which demonstrate that they comply with NAF’s high standards for safety and patient-centered care. Additionally, the nonprofit Power To Decide launched a digital abortion finder tool just last month that can help you safely find a verified physician or nurse practitioner in your area. This can be accessed at abortionfinder.org. If you know you won’t be able to pay for your abortion, NAF has a confidential hotline you can call to request help with funding: 1-800-772-9100. If they can’t cover you, try the National Network of Abortion Funds website, which lists organizations that help folks pay for their abortions, broken down by state. If your state doesn’t have a fund, call the one in the neighboring state, and they’ll likely know what to do. “If someone goes through the trouble to find us, we’ll rarely turn them away,” Roberts adds. Besides money for abortions, these funds may offer assistance with travel, hotels, and emotional support, too.Worth noting: Many abortion funds need financial support. If you’re able, consider donating to a fund using the resources above. “Any way people want to give money or resources, we’ll make it happen and find a way to take the donation, just reach out,” Roberts says. “Even if that means giving us a gift card you got for your birthday that you know you won’t use, everything helps.
Angel, now 21, is pregnant again — and this time, she’s thrilled. Her abortion allowed her to get back on her feet financially, and she says she has no regrets. She’ll forever be grateful for the emotional and physical support that Fund Texas Choice gave her as she traveled across state lines to take the abortion pill at five weeks. She remembers sipping a Sprite on her long drive home — a soda the fund’s program coordinator had bought her — knowing she’d made the right decision. And she feels even more confident in her choice today. “I’m much happier now,” she says. “Right now, if I wanted to have an abortion, I could actually afford to make that choice. My abortion helped open up doors to get me where I’m at now. It was something that needed to happen.”
*Angel’s name has been changed to protect her identity.










/https://static.texastribune.org/media/files/a7633b101c55f4a6d8153be23f19e3d7/Womens%20Health%20Clinic%20SS%20TT%2006.jpg)